Incontinentia Pigmenti with vesicular stage
Published Web Location
https://doi.org/10.5070/D39dz2p5bkMain Content
Letter: Incontinentia Pigmenti with vesicular stage in utero
Filipa Osório MD, Sofia Magina MD, Ana Nogueira MD, Filomena Azevedo MD
Dermatology Online Journal 16 (10): 13
Department of Dermatology and Venereology, Hospital de São João E.P.E., Porto, PortugalAbstract
Incontinentia pigmenti (IP) is a genodermatosis with a characteristic evolution of skin lesions. Most patients present with vesicles at birth or within the first weeks of life. We report a case of a female infant with genetically confirmed sporadic IP who presented with verrucous and hyperpigmented lesions with no previous vesicular stage.
Introduction
Incontinentia pigmenti (IP) is an uncommon X-linked dominant genodermatosis, associated with mutations in nuclear factor-kappa B (NF-κB) essential modulator (NEMO) gene [1]. There is ectodermal dysplasia, with involvement of the skin, hair, teeth, and nails, together with neurologic and ophthalmologic anomalies. Cutaneous lesions are typically observed at birth or within the first weeks of life, evolving in 4 sequential stages: (1) vesicular, (2) verrucous, (3) hyperpigmented, and (4) hypopigmented [2].
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Hyperpigmented lesions following Blaschko lines on the trunk (anterior aspect) Figure 2. Hyperpigmented lesions following Blaschko lines on the trunk (posterior aspect) | |
A female infant was born with hyperpigmented lesions following Blaschko lines on the trunk and limbs. Two weeks after birth she developed two verrucous plaques, one on the right lateral malleolus and the other on the 5th right finger. She was 1-month-old when she presented to our department. Physical examination did not reveal any other significant findings.
 |  |
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. Hyperpigmented lesions following Blaschko lines on the inferior limbs Figure 4. Verrucous plaque on the right lateral malleolus | |
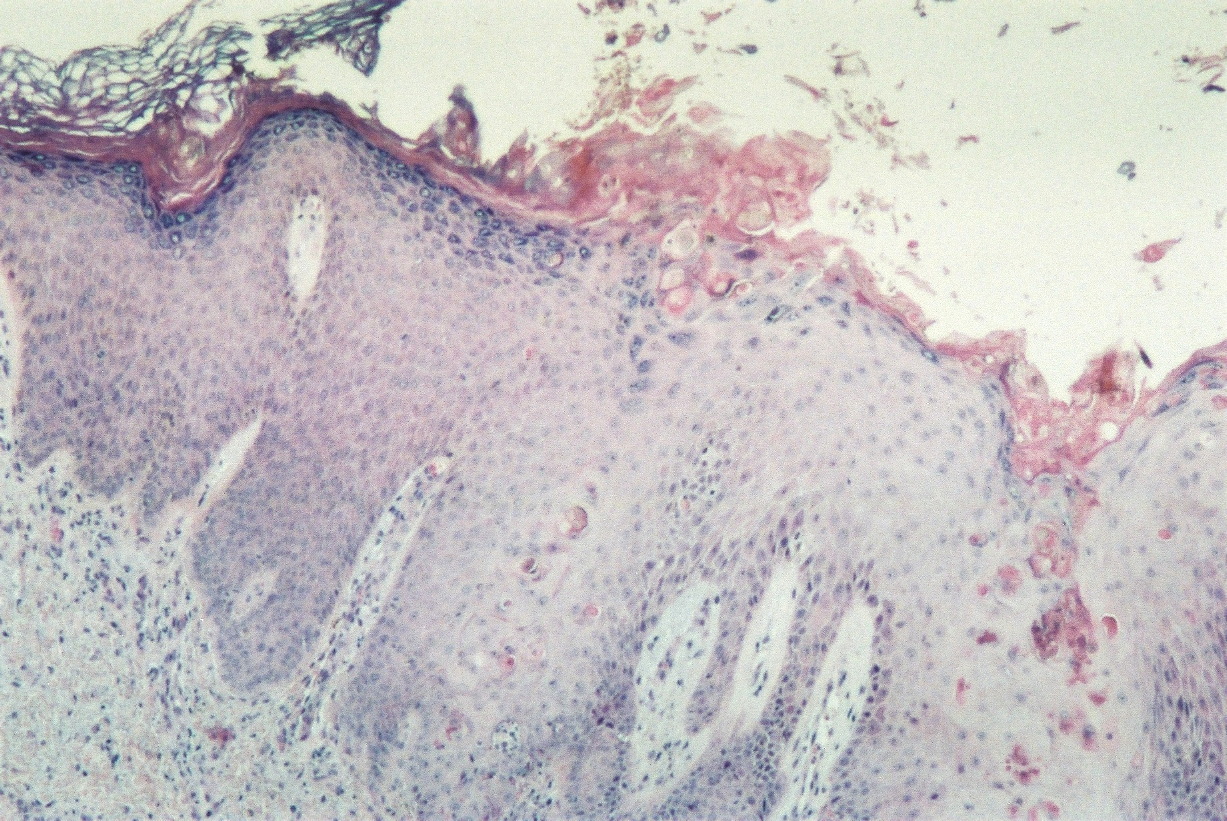
A biopsy of the hand lesion was made revealing acanthosis, hyperkeratosis, numerous apoptotic keratinocytes, focal superficial edema, and a sparse inflammatory infiltrate with the presence of eosinophils.
 |  |
| Figure 5 | Figure 6 |
|---|---|
| Figure 5. Verrucous plaque on the 5th right finger Figure 6. Histological picture of the hand verrucous lesion | |
Our diagnosis was IP with vesicular stage in utero and we requested a genetic study of the NEMO gene, which detected the common deletion involving exons 4-10 in the heterozygous state.
The mother presented with hypopigmented atrophic linear lesions on the chest, abdomen, buttocks, and thighs, which she believed had appeared during pregnancy and were clinically consistent with striae, but exhibited no other skin abnormalities. She also had a history of spontaneous abortion. However, the NEMO gene study was negative for any mutation.
The infant and her mother were then lost to follow-up because they went to live in another country.
Discussion
In IP, the vesicular stage is most frequently observed at birth or within the first two weeks of life, but it is absent in 5-10 percent of cases, in which it is believed to occur in utero [3, 4, 5]. This is what probably happened with our patient who presented with verrucous and hyperpigmented lesions.
Incontinentia pigmenti appears to be more common among white patients, but it has also been reported in other races, as in our patient who was of African heritage [6].
The mother’s hypopigmented lesions were initially interpreted as being either striae or IP hypopigmented lesions, which typically appear in adolescence after resolution of previous stages [2]. Although there was no information about the fetus’s sex, as IP is usually lethal in males, this could have explained the history of spontaneous abortion [7]. However, the mother’s genetic study was negative, so our patient’s skin is the result of a spontaneous mutation. In fact, according to the literature, family history is reported in 28-55.4 percent of the cases [3, 4].
The diagnosis of IP is initially based on clinical criteria. Skin biopsy may help if performed during the vesicular or verrucous stages. Eosinophils are often sparsely present in the verrucous stage (as in our patient), compared to the florid eosinophilic infiltrates in the vesicular stage. Eosinophilia may be noted during the vesicular stage. Neuroimaging is performed when neuro-ophthalmologic involvement is suspected [2, 6]. Although not strictly necessary, the NEMO gene study can confirm or rule out the diagnosis. Eighty to ninety percent of IP probands carry a common deletion comprising exons 4-10 of NEMO, as it was in our case [1, 4, 7].
Cutaneous lesions usually don’t require any treatment, but the patient should be monitored for the development of secondary cutaneous infections during the vesicular stage. Regular dental care is necessary. Anticonvulsivants must be used if the patient presents with seizures. Ophthalmologic surgery may be necessary. Prognosis is generally good and it is related to ophthalmologic and neurologic involvement [6].
Conclusion
Incontinentia pigmenti should be suspected in every infant who presents with verrucous and/or hyperpigmented lesions, even if there is no history of a previous vesicular stage. The NEMO gene study may help with the diagnosis in cases of clinical doubt.
References
1. Smahi A, Courtois G, Vabres P, Yamaoka S, Heuertz S, Munnich A, Israël A, Heiss NS, Klauck SM, Kioschis P, Wiemann S, Poustka A, Esposito T, Bardaro T, Gianfrancesco F, Ciccodicola A, D'Urso M, Woffendin H, Jakins T, Donnai D, Stewart H, Kenwrick SJ, Aradhya S, Yamagata T, Levy M, Lewis RA, Nelson DL. Genomic rearrangement in NEMO impairs NF-kappaB activation and is a cause of incontinentia pigmenti. The International Incontinentia Pigmenti (IP) Consortium. Nature. 2000 May;405(6785):466-72. [PubMed]2. Landy SJ, Donnai D. Incontinentia pigmenti (Bloch-Sulzberger syndrome). J Med Genet. 1993 Jan;30(1):53-9. [PubMed]
3. Carney RG. Incontinentia pigmenti. A world statistical analysis. Arch Dermatol. 1976 Apr;112(4):535-42. [PubMed]
4. Hadj-Rabia S, Froidevaux D, Bodak N, Hamel-Teillac D, Smah A, Touil Y, Fraitag S, Prost Y, Bodemer C. Clinical Study of 40 cases of incontinentia Pigmenti. Arch Dermatol. 2003 Sep;139(9):1163-70. [PubMed]
5. Vicente-Villa A, Lamas JV, Pascual AM, Cuesta DL, Marfa MP, González-Enseñat MA. Incontinentia pigmenti: a report of ten cases. Eur J Pediatr. 2001 Jan;160(1):64-5. [PubMed]
6. Berlin A, Paller AS, Chan LS. Incontinentia pigmenti: A review and update on the molecular basis of pathophysiology. J Am Acad Dermatol. 2002 Aug;47(2):169-190. [PubMed]
7. Phan T, Wargon O, Turner A. Incontinentia pigmenti case series: clinical spectrum of incontinentia pigmenti in 53 female and their relatives. Clin Exp Dermatol. 2005 Sep;30:474-80. [PubMed]
© 2010 Dermatology Online Journal