Familial leiomyomatosis cutis et uteri
Published Web Location
https://doi.org/10.5070/D37dr40688Main Content
Familial leiomyomatosis cutis et uteri
Christopher T Cassetty MD
Dermatology Online Journal 10 (3): 5
From the Ronald O. Perelman Department of Dermatology, New York University
Abstract
A 45-year-old woman presented with multiple, small, asymptomatic, hyperpigmented to skin-colored, smooth, dermal papules on the right temple as well as with uterine fibroids. She has a family history of uterine fibroids and cutaneous leiomyomas. An autosomal dominant disorder of multiple cutaneous leiomyomas and uterine fibroids (Reed syndrome) has been localized to a gene on chromosome 1q42.3-43. This gene encodes fumarate hydratase, which is an enzyme in the Kreb cycle, that acts as a tumor suppressor in this familial disorder. A subset of people may be at risk for papillary renal cell carcinoma.
History.—A 45-year-old woman complained of a 7-year history of papules on the right temple. The patient was evaluated at the Charles C. Harris Skin and Cancer Pavilion in September 2003 for a cluster of papules on her face; these lesions had increased in number over the last 7 years. The lesions were asymptomatic except for occasional prominence when experiencing goose flesh elsewhere on her body. Previous treatment with laser surgery had little effect. Past medical history includes symptomatic uterine fibroids for which a hysterectomy is scheduled. Her family history includes similar cutaneous lesions in one sister and uterine fibroids in all four sisters.
Physical Examination.—On the right temple were 2-3 mm, hyperpigmented to skin-colored, smooth, dermal papules agminated into a 4-cm plaque. A mechanical stroke was not associated with contraction of the papules or pain.

|
|
| Figure 1 | Figure 2 |
|---|
Laboratory Data.—An abdominal computerized-tomography scan performed in February 2003 showed uterine fibroids and normal kidneys.
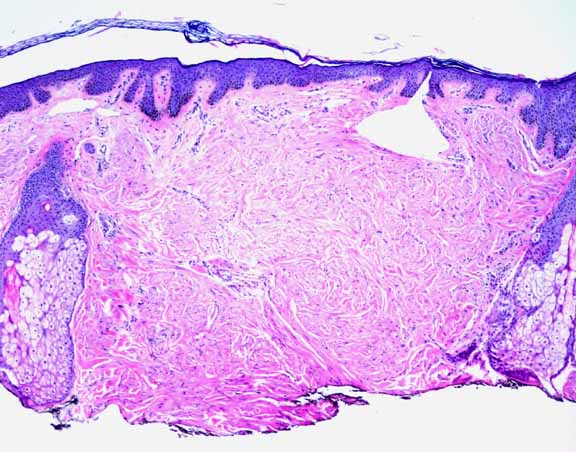
Histopathology.—There is proliferation of smooth-muscle bundles arranged as fascicles in the papillary and reticular dermis with mild nuclear atypia
Diagnosis.—Familial leiomyomatosis cutis et uteri (Reed syndrome).
Comment
Cutaneous leiomyomas are uncommon, benign, smooth muscle tumors that are divided into three categories: solitary or multiple piloleiomyomas arising from the arrectores pilorum; solitary genital piloleiomyomas arising from the smooth muscle of the areolae and dartos muscle of the genitalia; and angioleiomyomas arising from the vascular smooth muscle [1, 2].
Multiple piloleiomyomas are the most common type; they present in grouped, linear, or dermatomal patterns of firm, red, pink, brown, or skin-colored, dermal nodules. They involve (in descending order of frequency) the extensor surfaces of the extremities, the trunk, face, and neck [3]. There may be an association of pain with the piloleiomyomas and angioleiomyomas when exposed to cold, trauma, or pressure. They often appear in adolescence or early adulthood and may achieve 1-2 cm in size [1, 2, 3]. Histologically, piloleiomyomas are tumors with a poorly circumscribed, haphazard array of smooth-muscle fibers in the reticular dermis between collagen bundles and, at times, in the subcutaneous adipose tissue; often there is a thin grenz zone [1, 2, 3].
Leiomyomas occur sporadically, although multiple cutaneous leiomyomas may have an autosomal dominant inheritance [4]. An autosomal dominant disorder consisting of multiple cutaneous leiomyomas and uterine fibroids (Reed syndrome) has been localized to a gene on chromosome 1q42.3-43 [4]. This gene encodes fumarate hydratase, an enzyme in the Kreb cycle that acts as a tumor suppressor in this familial disorder. A subset of affected people may be at risk for papillary renal cell carcinoma [4].
Treatment of cutaneous leiomyomas is based on symptomatic or cosmetic concerns and is usually limited to excision of single lesions. Asymptomatic lesions are left untreated especially when multiple lesions are present, because of the likelihood of recurrence. Symptomatic lesions that are not amenable to resection are more difficult to treat. The etiology of pain in leiomyomas is unclear, but it is thought to be related to smooth-muscle contraction or compression of nerve bundles in larger tumors [5]. Therapeutic interventions include oral nitroglycerin, nifedipine, and phenoxybenzamine, which is aimed at relaxing smooth muscle, and topical analgesics for pain. [5]
References
1. Spencer JM, et al. Tumors with smooth muscle differentiation. Derm Surg 1996;22:761.2. Holst VA, et al. Cutaneous smooth muscle neoplasms: clinical features, histologic findings, and treatment options. J Am Acad Dermatol 2002;46:477.
3. Garman ME, et al. Familial leiomyomatosis: a review and discussion of pathogenesis. Dermatology 2003;207:210.
4. Multiple Leiomyoma Consortium. Germline mutations in FH predispose to dominantly inherited uterine fibroids, skin leiomyomata and papillary renal cell cancer. Nat Genet 2002;30:406.
5. Archer CB, et al. Pharmacological modulation of cold-induced pain in cutaneous leiomyomata. Br J Dermatol 1988;118:255.
© 2004 Dermatology Online Journal