The baboon syndrome or intertriginous drug eruption: A report of eleven cases and a second look at its pathomechanism
Published Web Location
https://doi.org/10.5070/D36qk5r7nvMain Content
The baboon syndrome or intertriginous drug eruption: A report of eleven cases and a second look at its pathomechanism
Ronni Wolf MD,1 Edith Orion MD, 1 and Hagit Matz MD 1, 2
Dermatology Online Journal 9 (3): 2
1. The Dermatology Unit, Kaplan Medical Center, Rechovot, Israel. 2. The Department of Dermatology, Tel-Aviv Sourasky Medical Center and the Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel. wolf_r@netvision.net.il
Abstract
Although drug eruptions can mimic a variety of idiopathic skin diseases, this has not been mentioned in the differential diagnosis of intertrigo. We draw attention to an unusual presentation of a drug eruption with a characteristic distribution pattern that is confined to the intertriginous areas. This condition has been given one of the most memorable names in dermatology, the baboon syndrome. Originally, the baboon syndrome was described as a special form of systemic contact-type dermatitis (SCTD) that occurs after ingestion or systemic absorption of a contact allergen in individuals previously sensitized by topical exposure to the same allergen in the same areas. We present eleven cases of intertriginous eruptions that resulted from adverse drug reactions. A flare-up of a previous contact with the same allergen (i.e., drug) on the same areas is not a reasonable explanation for the unusual localization of the eruption in our and others' cases. We believe that we are dealing with a type of recall phenomenon and that the characteristic localization and appearance of the eruption is determined by an earlier, unrelated dermatitis that had occurred in precisely the same areas. Adverse drug reactions should always be considered in the differential diagnosis of intertrigo, especially in atypical and therapy-resistant cases.
Introduction
Although drug eruptions can mimic a variety of skin diseases, intertrigo is generally easily distinguished from these. Awareness of this unusual drug reaction is especially important because the connection might be easily overlooked and misdiagnosed.
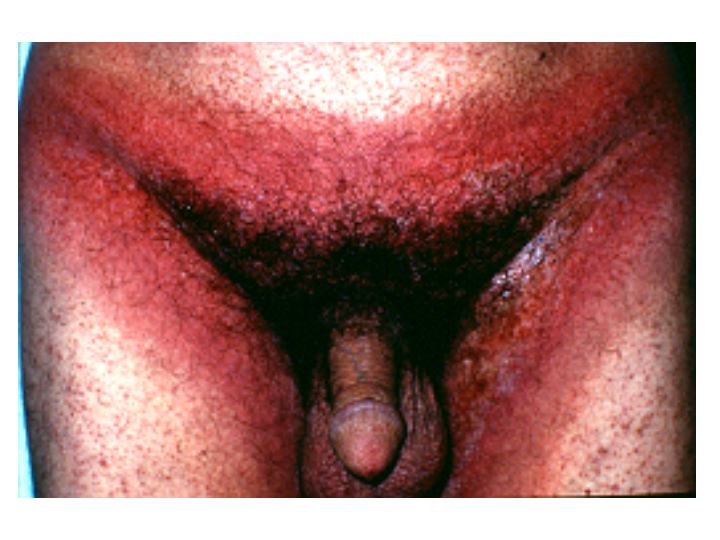
We present eleven cases of an unusual drug reaction confined to the intertriginous areas. We believe that they are identical to those reported as the baboon syndrome, a term used to describe bright-red, well-demarcated, anogenital lesions associated with a symmetric eczematous eruption involving axillae, antecubital fossae, eyelids, and the sides of the neck.[1]
We shall try to challenge the current concept that this syndrome represents a special form of hematogenous or systemic contact-type dermatitis (SCTD) and propose another more encompassing concept to explain the mechanism behind this bizarre form of drug eruption.
Report of cases
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Bullae between fingers of patient 1 (Figs. 1 and 2) | |
Case 1.—A 74-year-old man was referred from the internal medicine department where he was hospitalized for metastatic lung carcinoma. He had developed a bullous and erosive eruption confined to the intertriginous areas (e.g., genital, inguinal, perianal, and axillary areas and between the toes and fingers) 48 hours after he had received Percodan (a combination product containing oxycodone hydrochloride, oxycodone terephthalate and aspirin). On presentation, he had erosions confined to the inguinal, perianal and axillary areas, and bullae between his toes and fingers (Figs. 1, 2). Because the skin condition had not been diagnosed when it first appeared and was not considered as being related to the drug, Percodan was again given to the patient and the eruption reappeared in the same areas. He had been in a terminal stage when the eruption appeared and had received no other medications at the time. He died before any workup or laboratory investigation could be done.
 |  |
| Figure 3 | Figure 4 |
|---|---|
| Sharply demarcated erythema and erosion confined to the underpants area of patient 2 (Fig. 3). | |
| Erythema at the buttocks of patient 2 (Fig. 4). | |
Case 2.—A 60-year-old patient consulted us about an erythematous, purpuric, erosive eruption confined to three intertriginous areas (inguinal, buttocks, and axillae). The eruption mimicked intertrigo (Figs. 3, 4). The histological picture was consistent with the mixed dermal-epidermal type of erythema multiforme. A day before the appearance of the eruption, he had started to take naproxen tablets (Naxyn® 500 mg) for low back pain. He had received the same medication 2 months earlier for the same indication without any side effects. Withdrawal of the drug without any other therapy except for saline compresses to the affected skin was followed by a rapid improvement within 2 days and complete clearing of the eruption within one week. Patch tests, carried out with naproxen at concentrations of 1 percent, 2 percent, 5 percent, 10 percent and 20 percent, prepared in petrolatum and water as a vehicle similar to the method of Gonzalo et al., were negative at 48, 72 and 96 hours.[2]
 |
| Figure 5 |
|---|
| Erythematous eruption at the inner thighs of patient 3. |
Case 3.—A 28-year-old man developed an erythematous pruritic eruption affecting his inner thighs (Fig. 5), buttocks, and axillae 8 days after starting amoxicillin for an upper respiratory infection. He had taken penicillin in the past without any adverse effects. The eruption resolved completely after 1 week without any therapy. Patch testing was carried out with the European Standard Series and with Textile Color & Finish Series (both from Chemotechnique Diagnostics, Sweden), and with amoxicillin (5 percent, 10 percent and 30 percent in petrolatum and in water according to the guidelines of the International Contact Dermatitis Research Group and of Barbaud et al.), and the results were negative.[3, 4, 5]
 |
| Figure 6 |
|---|
| A red maculopapular rash with targetoid lesions in the inguinal area of patient 4. |
Case 4.—A 35-year-old man developed an erythematous eruption on his inner thighs and buttocks 4 days after he was put on a combination product of amoxicillin and clavulanic acid (Augmentin®) for a periodontal abscess. Examination revealed a light-red maculopapular rash symmetrically distributed on the buttocks and thighs (Fig. 6), which became confluent in some areas and showed some targetoid lesions on others. Augmentin® was replaced by clindamycin, and the lesions healed completely within 4 days.
 |
| Figure 7 |
|---|
| Erythematous eruption on inguinal/abdominal folds of patient 5. |
Case 5.—A 62-year-old man was referred from the department of surgery with an erythematous, purpuric eruption on the lower abdomen, inguinal folds (Fig. 7) and buttocks. The eruption had appeared 1 day after he had received intravenous amoxicillin and cloxacillin for treatment of postoperative fever. Despite discontinuation of the drugs, the eruption spread during the next few days and resembled an ampicillin reaction. There was a red maculopapular rash distributed on his trunk and extremities. The rash became confluent and resolved after 10 days without further therapy except hydroxyzine. A skin biopsy from a lesion on his buttocks showed edema in the papillary dermis and an inflammatory, mainly perivascular, lymphohistiocytic infiltrate with eosinophils in the papillary and reticular dermis. There was no involvement of the epidermis. PAS stains were negative for fungal elements.
 |
| Figure 8 |
|---|
| Intensive erythema sharply confined to the underpants area of patient 6. |
Case 6.—We were asked to evaluate a 64-year-old patient who was hospitalized in the intensive care unit for sepsis and multiorgan failure secondary to wound infection. He had developed an erythema of the groin area (Fig. 8) and his axillae 1 day after he was put on antibiotic therapy with ceftriaxone and ciprofloxacin. He had a history of penicillin allergy. The antibiotic therapy was changed to vancomycin, clindamycin, and gentamicin; however, the eruption spread until the patient become erythrodermic. The eruption cleared within a week from all areas without any specific therapy: he received no steroids, antihistamines, or any topical treatment.
 |
| Figure 9 |
|---|
| Patient 7 presenting erythema in the inguinal area. |
Case 7.—A 48-year-old woman developed a pruritic, symmetric erythema on her buttocks, inner thighs (Fig. 9) and axillae 8 days after she had received prophylactic cephalexin after undergoing a gynecological procedure. Her condition had been diagnosed clinically in an outpatient dermatologic clinic as candida intertrigo, and she was being treated with a cream containing isoconazole nitrate and diflucortolone valerate. She was sent to us for consultation because her skin condition failed to improve after 1 week of topical therapy. Her skin lesions completely resolved within 5 days after discontinuation of the drug.
 |
| Figure 10 |
|---|
| Erythema and erosions at the axilla of patient 8. |
Case 8.—A 62-year-old man received cefuroxime (Zinnat®) 500 mg twice daily for an upper respiratory infection. After being on this regimen for one day, he developed a symmetric erythematous rash in the axillary and inguinal areas. This rash was diagnosed as intertrigo and treated with a cream containing bifonazole 1 percent and fluocinonide 0.05 percent. When the eruption failed to respond and became even more inflamed with erosions and oozing, the topical medication was stopped and he was instructed to apply only wet saline compresses. When the patient was referred to us after having taken antibiotics for 9 days (Fig. 10), the possibility of a drug-induced eruption was considered, and he was instructed to discontinue his antibiotic. Within 2 days of withdrawal of the drug, the skin condition improved remarkably and cleared altogether within 10 days. Patch tests with cefuroxime and cephalexin at 30 percent in petrolatum and in water (according to the guidelines of Barbaud et al.) were negative.[4]
 |
| Figure 11 |
|---|
| Sharply demarcated erythema in the groin area of patient 9. |
Case 9.—An 83-year-old man was admitted to our clinic for evaluation of an erythematous pruritic rash of 12 days' duration in the inguinal (Fig. 11), and gluteal area. The patient's history revealed that he was generally in good health and that he had been started on cephalexin 500 mg four times daily for urinary tract infection 4 days prior to the appearance of the dermatitis. He had been allergic to penicillin for years. Withdrawal of cephalexin brought about a rapid improvement of the eruption until it cleared completely within 2 weeks, without any topical or systemic therapy.
Case 10.—A 79-year-old woman developed a pruritic, erythematous eruption of the inguinal (Fig. 12), gluteal, axillary, and inframammary areas within a few hours after she had received a barium sulphate-containing contrast media for gastrointestinal radiography. The eruption resolved spontaneously within 2 days.
 |  |
| Figure 12 | Figure 13 |
|---|---|
| Patient 10 showing bright red erythema in the inguinal area (Fig. 12). | |
| A circular, erythematous eruption on the axilla of patient 11 (Fig. 13). | |
Case 11—A 75-year-old woman was admitted because of an eruption confined to the intertriginous areas. This occurred 8 days after she was put on amoxicillin, clarithromycin, and omeprazole for the treatment of a Helicobacter-associated peptic ulcer. She had received no other medications and had no previous history of allergy. She was found to have a maculopapular, erythematous eruption that became confluent and was arranged in a circle surrounding normal skin in the axillary, inframammary, and inguinal areas (Fig. 13). The eruption cleared rapidly within a few days after withdrawal of the medications.
Discussion
The cases described above are not examples of typical irritant or candida-related intertrigo. All responded to withdrawal of drug without any topical therapy after this was done. Those patients who had previously been on topical steroids or antifungals had been unresponsive to these medications. When PAS stains were done on biopsied cases, they were negative. However, the eruptions and their typical courses are very similar to one another, and we believe that they are also similar to those reported as the baboon syndrome,[1] flexural exanthem,[6] or intertriginous drug eruption.[7, 8]
In 1984, Andersen et al. describe an eruption with a very characteristic distribution pattern provoked by several allergens such as ampicillin, nickel, and mercury.[1] This reaction pattern is labelled the baboon syndrome because of the characteristic, bright-red, well-demarcated eruption, predominantly located on the buttocks and genital areaóreminiscent of the red bottom of the baboon. They are convinced that this syndrome represents a special form of hematogenous or systemic contact-type dermatitis (SCTD). Other authors who later describe the syndrome [9, 10, 11, 12, 13] accept Andersen et al.'s hypothesis, which is still considered valid today without any further attempts to challenge its validity. [6, 14, 15, 16, 17, 18, 19,21, 22, 23, 24, 25, 26, 27, 28]
Hematogenous or SCTD is a type IV immunologic reaction triggered internally in patients previously sensitized to the same allergen by cutaneous exposure. [29, 30, 31, 32, 33] Although the eczematous condition is produced by systemic administration, the first sensitization has taken place by topical application (i.e., exogenous contact). Clinical symptoms appear in two different forms: (a) flare-up of earlier contact dermatitis lesions—these lesions are clinically and histopathologically indistinguishable from contact dermatitis and appear at the same sites of previous exposure, a mechanism proposed for the baboon syndrome; (b) various types of skin lesions appearing on skin not exposed to the hapten—these include dyshidrotic hand eczema, generalized maculopapular-vesicular rash, erythema multiforme, and vasculitis.
It is the intent of the current work to challenge the concept that the baboon syndrome represents a special form of SCTD that occurs after ingestion or systemic absorption of a contact allergen in individuals previously sensitized by topical exposure at the same areas. Andersen et al. [1] based their theory on the following facts:
(1)The eruption is demarcated by sharp, well-defined borders, as is contact dermatitis.
This observation appears to be the main reason Andersen et al. felt that it was a form of SCTD,[1] but it really does not justify the classification of the baboon syndrome as a SCTD. It is well known that drug eruptions can mimic a wide range of skin conditions. [34] The literature is replete with descriptions of many different drug reactions that are confined to specific, localized, well-demarcated areas of skin showing a particular geometric pattern (e.g., bleomycin-induced flagellate hyperpigmentation) [35, 36, 37, 38], the flag sign of chemotherapy [39], pustular eruption (Ofugi-like) on the face caused by ampicillin [40], acral erythema [41, 42, 43, 44, 45, 46, 47], chemotherapy-induced eccrine squamous syringometaplasia, or flexural erythematous eruption, characterized in most patients by well-defined erythema in the axilla and/or groin. [48, 49, 50, 51] Furthermore, other antigens, such as recently described bacterial toxins may cause a similar eruption but certainly not through any mechanism of contact dermatitis.[52, 53] It follows, then, that the distinct clinical appearance of the eruption is not sufficient proof of its being a form of contact dermatitis.
(2)The patch test is positive in most (although not all [9, 14, 54, 55]) cases of the baboon syndrome.
Positive patch tests are found in 25 percent of patients with various types of drug reactions to penicillin, [56, 57] and in 60 percent of patients with a fixed-drug eruption, [57, 58] In patch-testing patients with adverse drug reactions with a high likelihood of only one drug, Barbaud et al. found positive reactions in as many as 50 percent of 108 studied patients, although, as they recently stated, some of these results were false positive or irrelevant [59, 60]. A positive test, therefore, does not necessarily indicate contact dermatitis.
(3)Sensitivity to mercury and to nickel have been related to an eruption that develops following oral ingestion of these agents and also produces the baboon syndrome [5, 21, 61].
Although several of the described cases of the baboon syndrome [15, 19, 21, 62, 63] are probably manifestations of hematogenous or SCTD (i.e., the result of a flare-up of an eruption at exactly the same site of a previous sensitization with the same allergen), it seems very unlikely that this mechanism underlies most or even all of these described cases. Accepting the concept of SCTD as the responsible mechanism would mean that the patients have had previous contact with the offending drug at precisely the same areas of the eruption. This assumption is implausible for medications such as penicillin and synthetic penicillins, cephalosporins, analgesics, chemotherapeutics, and other drugs that are never included in topical preparations or put on the skin.
We propose another more encompassing concept to explain the mechanism behind this kind of drug eruption—one that would include SCTD as well. We consider that a recall phenomenon is responsible for the clinical manifestations of this bizarre form of drug eruption. Most cases of the baboon syndrome represent a recall of any form of dermatitis (unrelated to the drug currently in question) that had occurred in the past in the same areas as the new drug eruption. The previous dermatitis may have been severe diaper rash in infancy, contact dermatitis to any allergen or irritant, or other forms of typical intertrigo. If this be the case, then the agent causing the baboon syndrome is generally different and unrelated to the agent that had caused the dermatitis in the past, even though it might in specific cases be the same. The majority of these cases may then be compatible with the definition of Wolf's isotopic response. [64, 65, 66]
In summary, we do not feel that there is sufficient evidence to justify the inclusion of the baboon syndrome as a SCTD and that a flare-up of a previous contact with the same allergen (drug) on the same areas is a reasonable explanation for the unusual localization of the eruption in our and other investigator's cases. A kind of recall phenomenon, with the characteristic localization and appearance of the eruption determined by an earlier bout of dermatitis is a better, more universal, explanation. However, we applaud Andersen et al.'s recognition of this morphologic pattern and their choice of such a picturesque term.[1]
Whatever the theoretical considerations, the mechanism of this eruption and its classification and naming, it is vitally important to draw attention to clinical presentations of any drug eruption because these cases might be easily overlooked or misdiagnosed. We suggest that adverse drug reactions should always be considered in the differential diagnosis of intertriginous eruptions, especially in atypical and therapy-resistant cases.
Acknowledgment. Esther Eshkol is thanked for editorial assistance.
References
1. Andersen K, Hjorth N, Menne T. The baboon syndrome: Systemically-induced allergic contact dermatitis. Contact Dermatitis. 1984; 10: 97-100.2. Gonzalo M, Alvarado M, Fernandez L, Rosendo R, Gonzalez G. Fixed drug eruption due to naproxen; lack of cross-reactivity with other propionic acid derivatives. Br J Dermatol. 2001; 144: 1291-1292.
3. Lachapelle J, Ale S, Freeman S, et al. Proposal for a revised international standard series of patch tests. Contact Dermatitis. 1997; 36: 121-123.
4. Barbaud A, Reichert-Penetrat S, Trechot P, et al. The use of skin testing in the investigation of cutaneous adverse drug reactions. Br J Dermatol. 1998; 139: 49-58.
5. Barbaud A, Goncalo M, Bruynzeel D, Bircher A. Guidelines for performing skin tests with drugs in the investigation of cutaneous adverse drug reaction. Contact Dermatitis. 2001; 45: 321-328.
6. Wakelin S, Sidhu S, Orton D, Chia Y, Shaw S. Amoxycillin-induced flexural exanthem. Clin Exp Dermatol. 1999; 24: 71-73.
7. Wolf R, Brenner S, Krakowski A. Intertriginous drug eruption. Acta Derm Venereol (Stockholm). 1992; 72: 441-442.
8. Wolf R, Elman M, Brenner S. Drug-induced "intertrigo". Int J Dermatol. 1993; 32: 515-516.
9. Herfs H, Schirren C, Przybilla B, Plewig G. Das "Baboon-syndrome." Hautarzt. 1993; 44: 466-469.
10. Pfeiff B, Pullmann H. Baboon-artiges Arzeneiexanthem auf Heparin. Deutscher Dermatologe. 1991; 1991: 559-560.
11. Menne T, Weisman K. Haematogenes kontaktekzem nach oraler Gave von Neomyzin. Hautarzt. 1984; 35: 319-320.
12. Duve S, Worret W, Hofmann H. The baboon syndrome: a manifestation of haematogenous contact-type dermatitis. Acta Derm Venereol (Stockh). 1994; 74: 480-481.
13. Menne, T and Sjolin, KE. Systemic contact dermatitis: a model of unexplored clinical information. 1992. New York, 18th World Congress of Dermatology. (GENERIC) Ref Type: Conference Proceeding
14. Helmbold P, Hegemann B, Dickert C, Marsch W. Symmetric ptychotropic and nonpigmenting fixed drug eruption due to cimetidine (so-called baboon syndrome). Dermatology. 1998; 197: 402-403.
15. Guin J, Fields P, Thomas K. Baboon syndrome from I.V. aminophylline in a patient allergic to ethylenediamine. Contact Dermatitis. 1999; 40: 170-171.
16. Chowdhury M, Patel G, Inaloz H, Holt P. Hydroxyurea-induced skin diseases mimicking the baboon syndrome. Clin Exp Dermatol. 1999; 24: 336-337.
17. Panhans-Gross A, Gall H, Peter R. Baboon syndrome after oral penicillin. Contact Dermatitis. 1999; 41: 352-353.
18. Sanchez T, Sachez-Perez J, Aragues M, Garcia-Diez A. Flare-up reaction of pseudoephedrine baboon syndrome after positive patch test. Contact Dermatitis . 2000; 42: 312-313.
19. Bartolome B, Cordoba S, Sanchez-Perez J, Fernandez-Herrera J, Garcia-Diez A. Boboon syndrome of unusual origin. Contact Dermatitis . 2000; 43: 113
20. Kick G, Przybilla B. Delayed prick test reaction identifies amoxicillin as elicitor of baboon syndrome. Contact Dermatitis. 2000; 43: 366-367.
21. Audicana M, Bernedo N, Gonzalez I, Munoz D, Fernandez E, Gastaminza G. An unusual case of baboon syndrome due to mercury present in a homeopathic medicine. Contact Dermatitis. 2001; 45: 185
22. Strub C, Bircher A. Exanthema with emphasis of body flexure points 10 hours after administration of amoxicillin, "baboon syndrome". Schweiz Runsch Med Prax. 2002; 91: 232-234.
23. Amichai B, Grunwald M. Baboon syndrome following oral roxithromycin [Letter]. Clin Exp Dermatol. 2002; 27: 523
24. Cronin E. Ekzematose Reaktionen bei innerlicher Aufnahme von Kontaktallerenen. Hautarzt. 1975; 26: 68-71.
25. Kohler L, Schonlein K, Kautzky F, Vogt H. Diagnosis at first glance: the baboon syndrome. Int J Dermatol. 1996; 35: 502-503.
26. Le Coz C, Boos V, Cribier B, Grosshans E, Heid E. An unusual case of mercurial baboon syndrome. Contact Dermatitis. 1996; 35: 112
27. Isaksson M, Ljunggren B. Systemic contact dermatitis from ethylenediamine in an aminophylline preparation presenting as the baboon syndrome [Letter]. Acta Derm Venereol (Stockh). 2003; 83: 69-70.
28. Proske S, Uter W, Schnuch A, Hartschuh W. Severe allergic contact dermatitis with generalized spread due to bufexamac presenting as the "baboon" syndrome. Dtsch Med Wochenshcr. 2003; 128: 545-547.
29. Happle R. Paraptisches Ekzem. Hautarzt. 1994; 45: 1-3.
30. Cronin E. Reactions to contact allergens given orally or systematically. Br J Dermatol. 1972; 86: 104-107.
31. Fisher A. Systemic contact-type dermatitis. In: Fisher A, ed. Contact Dermatitis. Philadelphia, PA: Lea & Febiger; 1986: 119-129.
32. Menne T, Veien N, Maibach H. Systemic contact-type dermatitis due to drugs. Semin Dermatol. 1989; 8: 144-148.
33. Veien N. Systemically induced eczema in adults. Acta Derm Venereol (Stockh). 1989;Suppl 147: 1-58.
34. Wolf, R and Brenner, S. Drug induced dermatologic mimicry. 1993. Copenhagen- Denmark, 3rd EADV Congress. (GENERIC) Ref Type: Conference Proceeding
35. Cohen I, Master M, O'Keefe E, et al. Cutanrous toxicity of bleomycin therapy. Arch Dermatol. 1973; 107: 553-555.
36. Abig J, Gollnick H, Detmar M, Orfanos C. Flagellatartige hyperpigmentierung durch bleomycin. Hautarzt. 1992; 43: 376-379.
37. Tsuji R, Sawabe M. Hyperpigmentation in striae distensae after bleomycin treatment. J Am Acad Dermatol. 1993; 28: 503-505.
38. Yamamoto T, Yokizeki H, Nishioka K. Dermal sclerosis in the lesional skin of 'flagellate' erythema (scratch dermatitis) induced by bleomycin. Dermatology. 1998; 197: 399-400.
39. Wheeland R, Burgdorf W, Humphrey G. The flag sign of chemotherapy. Cancer. 1963; 51: 1356-1358.
40. Lim J, Ng S. An unusual drug eruption to ampicillin. Cutis. 1995; 56: 163-164.
41. Burgdorf W, Gilmore W, Garick R. Peculair acral erythema secondary to high-dose chemotherapy for acute myelogenous leukemia. Ann Intern Med. 1982; 97: 61-62.
42. Lokich J, Moore C. Chemotherapy associated palmar-plantar erythrodysesthesia syndrome. Ann Intern Med. 1984; 101: 798-800.
43. Jucgla A, Sais G, Navarro M, Peyri J. Palmoplantar keratoderma secondary to chronic acral erythema due to Tegaful. Arch Dermatol. 1995; 131: 364-365.
44. Ueki H, Namba M. Arzeneimittelexanthem durch ein neues 5-Rluorouracilderivat. Hautarzt. 1980; 31: 207-208.
45. Baack B, Furgdorf W. Chemotherapy-induced acral erythema. J Am Acad Dermatol. 1991; 24: 457-461.
46. Rios-Buceta L, Buezo G, Peoas P, Dauden E, Fernandez-Herrera J, Garcia-Diez A . Palmar-plantar erythrodysaesthesia syndrome and other cutaneous side-effects after treatment with Tegafur. Acta Derm Venereol (Stockh). 1997; 77: 80-81.
47. Azurdia R, Clark R, Friedmann P. Chemotherapy-induced acral erythema (CIAE) with bullous reaction. Clin Exp Dermatol. 1999; 24: 64-66.
48. Prussick R, Horn T, Wilson W, Turner M. A characteristic eruption associated with ifosfamide, carboplatin, and etoposide chemotherapy after pre-treatment with recombinant interleukin-1a. J Am Acad Dermatol. 1996; 35: 705-709.
49. Valks R, Fraga J, Porras-luque J, Figuuera A, Garcia-Diez A, Fernandez-Herrera J. Chemotherapy-induced eccrine squamous syringometaplasia. A distinctive eruption in patients receiving hematopoietic progenitor cells. Arch Dermatol. 1997; 133: 873-878.
50. Lotem M, Hubert A, Lyass O, et al. Skin toxic effects of polyethylene glycol-coated liposomal doxorubicin. Arch Dermatol. 2000; 136: 1475-1480.
51. Brazzelli V, Ardigo M, Chiesa M, et al. Flexural erythematous eruption following autologous peripheral blood stem cell transplantation: a study of four cases. Br J Dermatol. 2001; 145: 490-495.
52. Maders S, Heymann W, Atillasoy E, Kleeman J, Schlievert P. Recurrent toxin-mediated perineal erythema. Arch Dermatol. 1996; 132: 57-60.
53. Ichimiya M, Hamamoto Y, Muto M. A case of baboon syndrome associated with group a streptococcal infection. J Dermatol. 2003; 30: 69-71.
54. Barbaud A, Trechot P, Granel F, et al. A baboon syndrome induced by intravenous human immunoglobulins: report of a case and immunological analysis. Dermatology. 1999; 199: 258-260.
55. Weiss J, Mockenhaupt M, Schopf E, Simon J. Reproducible drug examthema to terbinafine with characteristic distribution of baboon syndrome. Hautarzt. 2001; 52: 1104-1106.
56. Bruynzeel D, Von Blomberg-van der Flier M, Scheper Real. Allergy for penicillin and the relevance of epicutaneous tests. Dermatologica. 1985; 171: 429-434.
57. Bruynzeel D, Van Ketel W. Parch testing in drug erupitons. Semin Dermatol. 1989; 8: 196-203.
58. Alanko K, Stubb S, Reitamo S. Topical provocation of fixed drug eruption. Br J Dermatol. 1987; 116: 561-567.
59. Barbaud A, Bene M, Faure G, Schmutz J. Tests cutanes dans l'exploration des toxidermies supposees de mecanisme immuno-allergique. Bull Acad Natle Med. 2000; 184: 47-63.
60. Barbaud A, Trechot P, Reichert-Penetrat S, Commun N, Schmutz J. Relevance of skin tests with drugs in investigating cutaneous adverse drug reactions. Contact Dermatitis. 2001; 45: 265-268.
61. Nakayama H, Niki F, Shono M, Hada S. Mercury exanthem. Contact Dermatitis . 1983; 9: 411-417.
62. Fernandez L, Maquiera E, Garcia-Abujeta J, et al. Baboon syndrome due to mercury sensitivity. Contact Dermatitis. 1995; 33: 56-57.
63. Gallo R, Parodi A. Baboon syndrome from 5-aminosalicylic acid. Contact Dermatitis. 2002; 46: 110
64. Wolf R, Brenner S, Ruocco V, Filioli F. Isotopic response. Int J Dermatol. 1995; 102: 341-348.
65. Tuzun Y, Iscimen A, Goksugur N, Demirkesen C, Tuzun B. Wolf's isotopic response: Trichophyton rubrum folliculitis appearing on a herpes zoster scar. Int J Dermatol. 2000; 39: 766-768.
66. Ruocco V, Ruocco E, Ghersetich I, Bianchi B, Lotti T. Isotopic response after herpesvirus infection: An update. J Am Acad Dermatol . 2002; 46: 90-94.
© 2003 Dermatology Online Journal