Porokeratosis of Mibelli: Successful treatment with 5 percent topical imiquimod and topical 5 percent 5-fluorouracil
Published Web Location
https://doi.org/10.5070/D36dg5m8j8Main Content
Porokeratosis of Mibelli: Successful treatment with 5 percent topical imiquimod and topical 5 percent 5-fluorouracil
Sangeetha Venkatarajan MD1, Todd M LeLeux MD2, Deborah Yang MD1, Theodore Rosen MD1, Ida Orengo MD1
Dermatology Online Journal 16 (12): 10
1. Department of Dermatology2. Department of Pathology
Baylor College of Medicine, Houston, Texas. iorengo@bcm.edu
Abstract
Porokeratosis of Mibelli (PM) is a clonal disorder of keratinization. It clinically presents with one or more annular plaques with central atrophy and elevated keratotic borders. With a 7.5 percent risk of malignancy, PM should be treated to prevent transformation into squamous cell carcinoma, Bowen disease, or basal cell carcinoma. Multiple treatment options are available, however, there is not one universally effective treatment. We describe the successful treatment of porokeratosis of Mibelli of the left calf in an 83-year-old man with topical 5 percent imiquimod and topical 5 percent 5-fluorouracil.
Case report
An 83-year-old man with a past medical history of coronary artery disease presented with a 1½-year history of a hyperpigmented annular plaque with central atrophy on his left calf (Figure 1). The lesion gradually grew to its current size of 2 cm indiameter over the prior 6 months but was without tenderness, pain, redness, warmth, or pruritus. At the time of examination, a second 2 cm round lesion on the right calf was confirmed to be superficial basal cell carcinoma by a shave biopsy. The affected areas had not undergone prior treatments. He denied a history of porokeratosis.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Clinical photograph of the patient’s left calf before treatment. Note the erythematous discoid plaques with peripheral
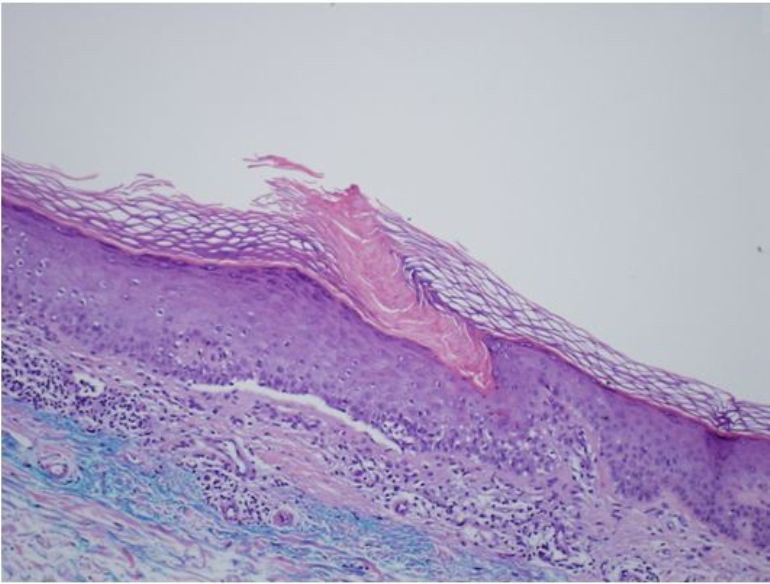
hyperpigmentation. Figure 2. Hematoxylin and Eosin stained section (100X) from our patient illustrating a column of parakeratosis, dyskeratotic keratinocytes, and a band-like lymphocytic infiltrate in the dermis. | |
The patient’s clinical history and physical exam suggested porokeratosis of Mibelli. A shave biopsy of the plaque on the left calf was performed. Histopathologic examination demonstrated a mildly acanthotic epidermis with columns of parakeratosis overlying dyskeratotic keratinocytes with absence of an intervening granular layer. A lichenoid lymphocytic infiltrate was also seen in the superficial papillary dermis (Figure 2). The histopathologic findings were consistent with porokeratosis.
The porokeratosis plaque on his left calf was initially treated with topical 5 percent 5-fluorouracil every morning and topical 5 percent imiquimod at night for 4 weeks. The treatment was modified because of the lack of response to initial treatment. Subsequently he was advised to apply topical 5 percent imiquimod in the morning and both topical 5 percent 5-fluorouracil and topical 5 percent imiquimod at night for four additional weeks. On follow-up, the annular plaque on the patient’s left calf appeared erythematous and irritated (Figure 3). The patient continued the treatment for 8 additional weeks. On examination, the treated area appeared well healed with mild residual hyperpigmentation after a total of 16 weeks (Figure 4).
 |  |
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. Clinical photograph of the patient’s left calf after 8 weeks of treatment. Note the erythematous and inflamed appearance
of the annular plaque. Figure 4. Clinical photograph of the patient’s left calf after 16 weeks of treatment. Note the resolution of the annular plaque with only mild scaling and minimal erythema present. | |
Discussion
Porokeratosis is a clonal disorder of keratinization and usually consists of 1 or more atrophic plaques bordered by a hyperkeratotic ridge-like border. There are five clinical variants of porokeratosis: classic porokeratosis of Mibelli, disseminated superficial actinic porokeratosis, porokeratosis palmaris et plantaris disseminata, linear porokeratosis, and punctate porokeratosis [2]. Our patient presented with a clinical presentation of PM.
Porokeratosis of Mibelli classically presents with one or multiple annular plaques with central atrophy and elevated keratotic borders that have a longitudinal furrow [2]. It commonly develops on the extremities but has also been known to occur on the face, palms and soles, genitalia, and buccal mucosa [3]. Histopathologically, PM has the cornoid lamella, a column of parakeratosis arising within the invagination of the epidermis. The granular layer is focally diminished and keratinocytes are dyskeratotic [4].
Porokeratosis of Mibelli has been associated with an increased risk of malignant transformation into squamous-cell carcinoma and Bowen disease, as well as basal-cell carcinoma [3], with rates as high as 7.5 percent. As a result, treatment is necessary when PM is diagnosed. Potential therapies include topical 5-fluorouracil, CO2 laser ablation, 585-nm pulsed dye laser radiation, oral retinoids, Grenz ray radiation, Nd:YAG laser radiation, cryotherapy, dermabrasion, surgical excision, electrodesiccation, and imiquimod [1].
A fluorinated pyrimidine, 5-fluorouracil, disrupts DNA synthesis by disrupting thymidine synthesis. This leads to cytotoxic activity towards rapidly dividing cells in the S phase. Because of the hyperproliferative nature of porokeratosis, topical 5-fluorouracil produces an inflammatory response [5]. Both topical as well as systemic 5-fluorouracil have been shown to be efficacious in the treatment of porokeratosis [5, 6].
Imiquimod induces the production of cytokines, which in turn stimulate Th-1 cells. This results in increased innate and acquired cellular immune responses. Because porokeratosis has been known to occur in cases of immunosuppression, there is a rational basis for the use of imiquimod [7]. Multiple published case reports of PM treated with 5 percent topical imiquimod have documented its efficacy [7, 8, 9]. Occlusion of the lesion was an important factor leading to resolution of the lesion in all 3 cases reported above. In our case, we treated the lesion with both imiquimod and 5-fluorouracil without occlusion, which produced complete resolution.
This report describes a patient with PM on the left calf treated with topical 5 percent imiquimod and topical 5 percent 5-fluorouracil, which resulted in complete resolution. We conclude that treatment with topical 5 percent imiquimod and topical 5 percent 5-fluorouracil is another therapeutic option for PM. Further investigation of the efficacy, tolerability, and side effects of imiquimod and 5-fluorouracil in PM is needed.
References
1. Montes-De-Oca-Sanchez G, Tirado-Sanchez A, Garcia-Ramirez V. Porokeratosis of Mibelli of the axillae: Treatment with topical imiquimod. J Dermatolog Treat. 2006:17(5): 319-20. [PubMed]2. Pizzichetta MA, Canzonieri V, Massone C, Soyer HP. Clinical and Dermoscopic Features of Porokeratosis of Mibelli. Arch Dermatol. 2009;145(1): 91-92. [PubMed]
3. Kanitakis J, Euvrard S, Faure M, Claudy A. Porokeratosis and immunosuppression. Eur J Dermatol. 1998;8(7): 459-65. [PubMed]
4. Alexis AF, Busam K, Myskowski PL. Porokeratosis of Mibelli following bone marrow transplantation. Int J Dermatol. 2006;45(4): 361-5. [PubMed]
5. Nahm WK, Donohue KG, Danahy IF, Badiavas E, FAlanga V. Systemic 5-fluorouracil producing an inflammatory response in porokeratosis. J Eur Acad Dermatol Venereol. 2003;17(2):190-192. [PubMed]
6. McDonald SG, Peterka ES. Porokeratosis (Mibelli): Treatment with topical 5-fluorouracil. J Am Acad Dermatol. 1983;8(1):107-110. [PubMed]
7. Jain S. Successful treatment of porokeratosis of Mibelli with imiquimod 5% cream. Clin Exp Dermatol. 2006;31(2): 302-3. [PubMed]
8. Harrison S, Sinclair R. Porokeratosis of Mibelli: Successful treatment with topical 5% imiquimod cream. Australas J Dermatol. 2003;44(4): 281-283. [PubMed]
9. Agarwal S, Berth-Jones J. Porokeratosis of Mibelli: successful treatment with 5% imiquimod cream. Br J Dermatol. 2002;146(2): 331-344. [PubMed]
© 2010 Dermatology Online Journal