Verrucous carcinoma of the foot affecting the bone: Utility of the computed tomography scanner
Published Web Location
https://doi.org/10.5070/D35xc0n92sMain Content
Verrucous carcinoma of the foot affecting the bone: Utility of the computed tomography scanner
J García-Gavín, D González-Vilas, L Rodríguez-Pazos, D Sánchez-Aguilar, J Toribio
Dermatology Online Journal 16 (2): 8
Department of Dermatology, University Hospital Complex, Faculty of Medicine, University of Santiago de Compostela, Spain.
juangavin@gmail.comAbstract
Verrucous Carcinoma (VC) of the foot often affects deep structures such as tendons, muscles or bone. The complete removal of the tumor is essential to avoid recurrences. Radiological studies should be performed before surgical planning in order to determine the extent of the tumor. A 54-year-old man presented with a VC of the foot. Magnetic resonance imaging (MRI) demonstrated a soft-tissue mass affecting the plantar aponeurosis and the sole muscles, without evidence of bone invasion. Computed tomography (CT) showed a lytic area with cortical disruption in the fourth metatarsal neck. A transmetatarsal amputation was performed. Histopathological examination confirmed the bone invasion. MRI is considered the imaging technique of choice in studying VC of the foot. Computed tomography is superior to MRI in determining minimum changes in the cortical bone related to tumor invasion. We conclude that when MRI images are not conclusive, CT scan is a good alternative to determine incipient bone invasion.
Introduction
Verrucous Carcinoma (VC) of the foot often affects deep structures such as tendons, muscles or bone. The complete removal of the tumor is essential to avoid recurrences. Radiological studies should be performed before surgical planning. This is necesary to determine the extent of the tumor.
Case report
A 54-year-old man with a 2-year history of a warty mass on the sole of his left foot was seen in our Dermatology Service. The lesion had been diagnosed as a viral wart one year earlier. It had been treated with liquid nitrogen cryotherapy without success. In the last 6 months, the tumor gradually enlarged and spread making walking difficult.
Physical examination revealed a well-demarcated tumor affecting the ball of the foot. It consisted of a grey-brown exophytic and hyperkeratotic mass, which discharged malodorous debris through several sinus tracts (Figure 1).
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. An exophytic and hyperkeratotic mass that discharged malodorous debris through several sinus tracts Figure 2. Projections of well-differentiated epithelium extended into the dermis and deeper structures. There is an edematous stroma with a moderate lymphohistiocytic infiltrate. | |
Microscopically, the tumor exhibited both exophytic and endophitic growth patterns. A massively hyperplastic epidermis was demonstrated. There was marked hyperkeratosis with foci of parakeratosis. The granular layer was prominent and many cells were vacuolated, resembling the koilocytes of viral warts. There was minimal dysplasia. Projections of well-differentiated epithelium extended into the dermis and deeper structures, forming sinuses and keratin filled cysts. In the dermis there was an edematous stroma with a moderate lymphohistiocytic infiltrate. These findings were consistent with the diagnosis of verrucous carcinoma of the foot (Figure 2).
 |
| Figure 3 |
|---|
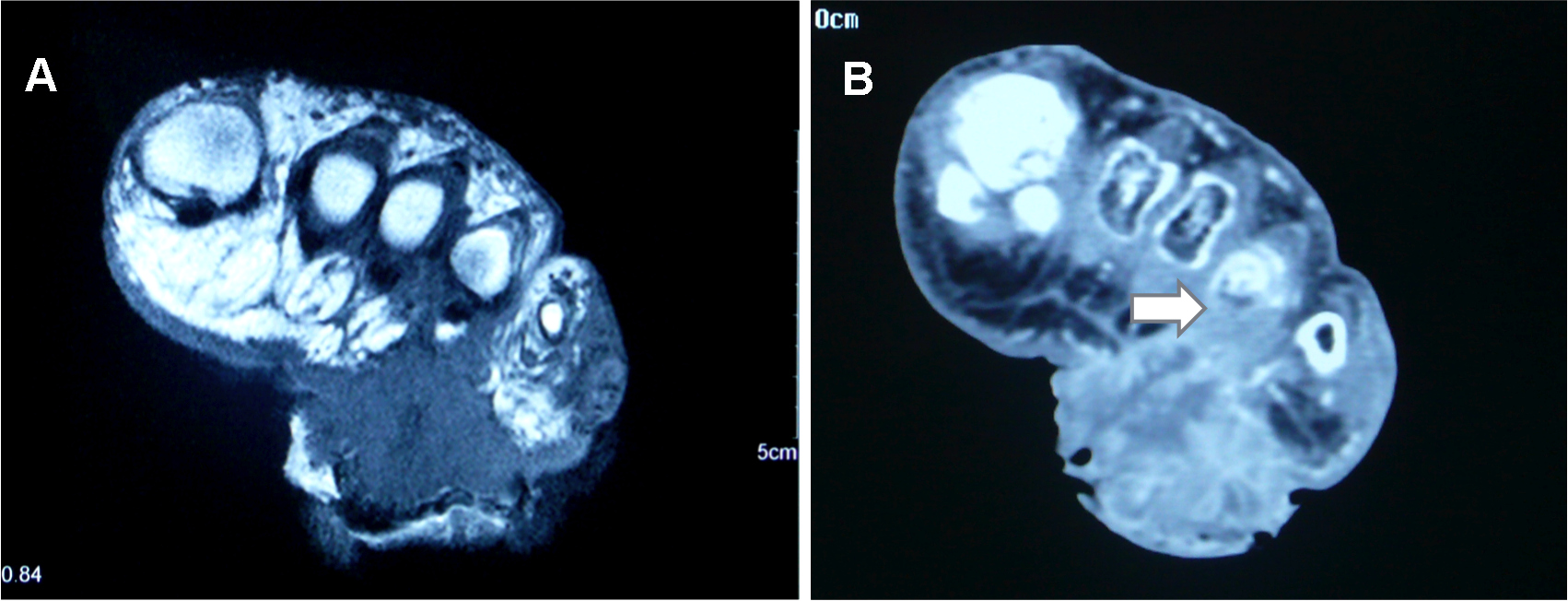
| Figure 3. (a) MRI: Tumor close to bone structures within images, suggestive of bone invasion (b) CT-scan: A lytic area with cortical disruption in the fourth metatarsal neck |
In order to define the extent of the lesion, a magnetic resonance imaging (MRI) was performed. The slides showed a soft-tissue mass affecting the outer side of the foot which extended proximally between the head of the metatarsals to 4 cm. Deep invasion affecting the plantar aponeurosis and the sole muscles was demonstrated. Although the mass was close to bone structures, there were no images suggestive of bone invasion. Computed tomography (CT) was then performed. A lytic area with cortical disruption in the fourth metatarsal neck was revealed, confirming an incipient bone invasion (Figure 3).
Transmetatarsal amputation of the third, fourth and fifth metatarsal was the surgical technique of choice. The histopathological study confirmed the bone involvement. One year later, the patient was able to walk with the aid of a prosthesis and there were no signs of recurrence.
Discussion
Verrucous carcinoma (VC) of the foot is an uncommon low-grade variant of squamous cell carcinoma characterized by local aggressive clinical behavior but a low potential for metastasis. It occurs mainly in men. The patients are predominantly older, with a mean age of 52 to 60 years. It is most often seen on the sole. The ball of the foot is the most frequent location [1].
Verrucous carcinoma of the foot usually appears as a warty tumor that may resemble verruca vulgaris. For that reason, many patients are initially treated with many topical medications without success [2]. The tumor tends to evolve as a soft-exophytic nodule, which expands into a bulky mass. Both exophytic and endophytic features may coexist, and if the latter is predominant, the lesion may extend into deeper structures. Such tumors often cause architectural distortion of adjacent tissues with destructive local invasion of tendons, muscle and even bone [3].
The basic approach to this tumor is surgical. Positive surgical margins have been related to worse prognosis [4]. Due to its endophytic growth, clinical assessment of the lesion extent is difficult. Radiological studies should be performed in order to confirm the presence of extracutaneous extension and determine which foot compartments are involved [5].
Bhushan et al. first reported the usefulness of MRI in the study of VC of the foot in 2001 [6]. They suggested that MRI may be the imaging technique of choice because it could discriminate between different types of soft tissue pathology. It may also be useful to determine the degree of involvement of muscle, fat, joint space, and neurovascular structures. However, MRI is not very sensitive for the identification of cortical lesions and periosteal reaction, so incipient bone invasion may be misdiagnosed [7].
Although CT is not routinely used to evaluate neoplastic lesions of the foot, it is superior to MRI in determining minimal changes in the cortical bone related to tumor invasion [8]. Computed tomography scanning has been successfully used in the diagnosis of bone involvement in VC in other locations [9, 10].
In this report, CT demonstrated a cortical bone invasion that was confirmed by histopathological examination. This finding determined a more aggressive surgical approach. A transmetatarsal amputation was required in order to remove the tumor and invaded tissues. We conclude that CT is a good alternative to detect cortical bone invasion when MRI images are not conclusive.
References
1. Schwartz RA. Verrucous carcinoma of the skin and mucosa. J Am Acad Dermatol 1995;32:1-21. [PubMed]2. Halpern J, Harris S, Suarez V, Jeyaratnam R, Smith AG. Epithelioma cuniculatum: A case report. Foot Ankle Surg 2009;15:114-6. [PubMed]
3. Ackerman LV. Verrucous carcinoma of the oral cavity. Surgery 1948;23:670-8. [PubMed]
4. Walvekar RR, Chaukar DA, Deshpande MS, Pai PS, Chaturvedi P, Kakade A, Kane SV, D'Cruz AK. Verrucous carcinoma of the oral cavity: a clinical and pathological study of 101 cases. Oral Oncol 2009;45:47-51. [PubMed]
5. Wasserman PL, Taylor RC, Pinillia J, Wuertzer SD. Verrucous carcinoma of the foot and enhancement assessment by MRI. Skeletal Radiol 2009;38:393-5. [PubMed]
6. Bhushan M, Ferguson JE, Hutchinson CE, Muston HL. Carcinoma cuniculatum of the foot assessed by magnetic resonance scanning. Clin Exp Dermatol 2001;26:419-22. [PubMed]
7. Taljanovic MS, Hunter TB, Fitzpatrick KA, Krupinski EA, Pope TL. Musculoskeletal magnetic resonance imaging: Importance of radiography. Skeletal Radiol 2003;32:403-11. [PubMed]
8. Johnson PT, Fayad LM, Frassica FJ, Fishman EK. Computed tomography of the bones of the foot: Neoplastic disease. J Comput Assist Tomogr 2009;33:436-43. [PubMed]
9. Aydogan LB, Ozdemir S, Gumurdula D. Verrucous carcinoma of the temporal bone. Am J Otolaryngol 2008;29:69-71. [PubMed]
10. Mucha SM, Stenson KM, Recant W, Naclerio RM. Radiology quiz case 2. Verrucous carcinoma of the maxillary antrum. Arch Otolaryngol Head Neck Surg 2003;129:259-61. [PubMed]
© 2010 Dermatology Online Journal