Epidermal nevus
Published Web Location
https://doi.org/10.5070/D34v4040s4Main Content
Epidermal nevus
Mercedes E Gonzalez MD, Ali Jabbari MD PhD, Brook E Tlougan MD, Rajni Mandal MD, Julie V Schaffer MD
Dermatology Online Journal 16 (11): 12
Department of Dermatology, New York University, New York, New YorkAbstract
A healthy 25-year-old man presented with a widespread, non-organoid, non-epidermolytic epidermal nevus. In addition to extensive hyperpigented patches and thin plaques following Blaschko lines, there were superimposed psoriasiform plaques on the elbows and warty plaques on the upper trunk. Striate palmar keraoderma also was evident. We review the clinical morphologies, sites of involvement, histopathologic findings (presence or absence of epidermolytic hyperkeratosis), and syndromal associations of non-organoid EN with underlying mutations in different genes.
History
 |  |
| Figure 1 | Figure 2 |
|---|
 |
| Figure 3 |
|---|
A 25-year-old man presented to the Dermatology Clinic at Bellevue Hospital Center for evaluation of widespread, hyperpigmented plaques. The lesions had been apparent since infancy, and over time they gradually had became darker and more noticeable. During adolescence, multiple, warty foci developed within the plaques. These areas temporarily became flatter and smoother when treated with clobetasol ointment occlusion. The patient denied associated pruritus, blisters, or erosions. He was otherwise healthy, with normal growth and development, and had no family history of skin disorders.
Physical examination
In a widespread distribution on the trunk, neck, and upper extremities, there were hyperpigmented patches and thin plaques that formed steaks and swirls along the lines of Blaschko. Superimposed upon these affected areas were several, discrete, thick, keratotic papules and plaques, which had a verrucous appearance on the upper trunk, and were sharply demarcated and pink with adherent, white scale on the elbows. Linear, yellow-brown, keratotic plaques extended from the wrist to the fingertips on the palms. The hair and nails were normal.
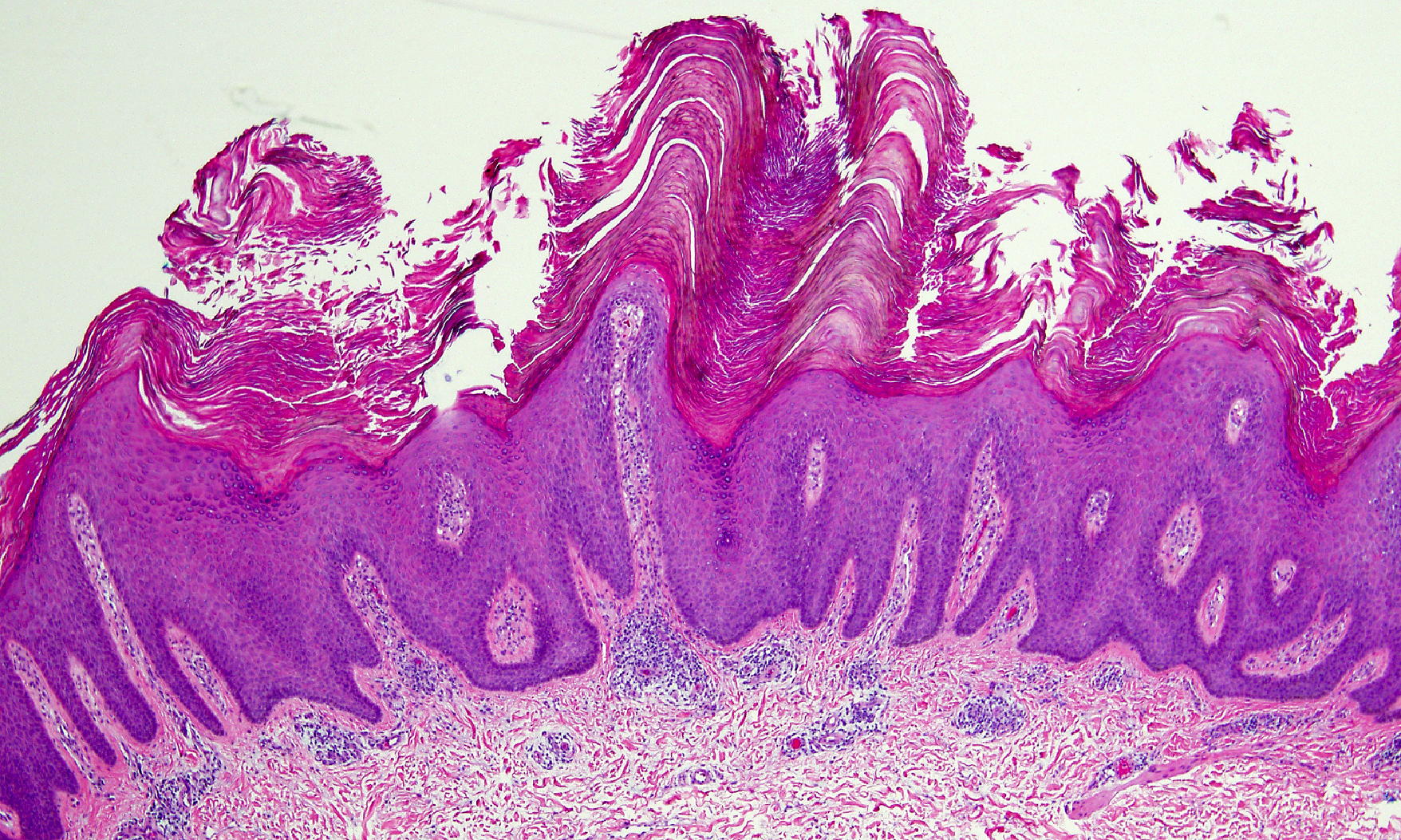
Histopathology
There is papillated epidermal hyperplasia, with hypergranulosis and hyperkeratosis that is composed of compact ortho- and parakeratosis.
Comment
Classic epidermal nevi (EN) are hamartomas with a Blaschkolinear configuration that reflects cutaneous mosaicism. These lesions result from a postzygotic mutation (or another genetic alteration) in an embryonic cell that is destined to populate an area of the epidermis, and Blaschko lines represent the pattern in which such keratinocyte precursor cells migrate and proliferate. Mutations that arise very early in embryonic development lead to more extensive EN and may affect organ systems other than the skin. When EN occur in conjunction with extracutaneous abnormalities, the term EN syndrome is used [1].
EN with prominent adnexal (sebaceous, follicular, and/or apocrine) differentiation are referred to as organoid nevi, and those with primarily epidermal differentiation are known as non-organoid or keratinocytic EN. Keratinocytic EN is usually present at birth or occurs during infancy as skin-colored or pink-to-hyperpigmented, Blaschkolinear streaks and swirls, which can be localized or widespread in distribution. The lesions initially may be flat and subtle; they tend to become more elevated and darker over time [1] The clinical morphologies, sites of involvement, histopathologic findings, and syndromal associations of keratinocytic EN vary depending upon the underlying genetic defect (Table 1) [2-8].
Our patient’s non-epidermolytic keratinocytic EN had several distinct morphologies, which included striate palmar keratodoma, psoriasiform plaques on the elbows, and warty plaques on the upper trunk as well as widespread hyperpigmented patches and thin plaques following Blaschko lines. This constellation of findings does not closely match that of any of the keratinocytic EN variants described in the Table. However, it is reminiscent of the non-epidermolytic palmoplantar keratoderma (diffuse or striate), sharply demarcated keratotic plaques on the elbows and knees, keratotic papules on the upper trunk, and variably generalized involvement that characterize ichthyosis hystrix of the Curth-Macklin (IHCM), which is an autosomal dominant disorder that is caused by mutations in the V2 domain of the keratin 1 (KRT1) gene [9]. Although the binucleate cells and perinuclear halos that represent the histopathologic hallmarks of IHCM were not evident in biopsy specimens from our patient, we have postulated that he may have a mosaic variant of IHCM and have pursued analysis of the KRT1 gene in lesional epidermis. Considering recent studies that show that human papillomavirus (HPV) DNA is prevalent in sebaceous nevi [10], which commonly develop warty changes around puberty, we also are testing for HPV in warty plaques from our patient.
References
1. Sugarman JL. Epidermal nevus syndromes. Sem Cutan Med Surg 2007; 23:145 [PubMed]2. Paller AS, et al. Genetic and clinical mocaiscism in a type of epidermal nevus. N Engl J Med 1994; 331:1408 [PubMed]
3. Tsubota A, et al. Keratin 1 gene mutation detected in epidermal nevus with epidermolytic hyperkeratosis. J Invest Dermatol 2007; 127:1371 [PubMed]
4. Terrinoni A, et al. A mutation in the V1 Domain of K16 is responsible for unilateral palmoplantar verrucous nevus. J Invest Dermatol 2000; 114:1136 [PubMed]
5. Hafner C, et al. Mosaicism of activation FGFR3 mutations in human skin causes epidermal nevi. J Clin Invest 2006; 116: 2201 [PubMed]
6. Hafner C, et al. Oncogenic PIK3CA mutations occur in epidermal nevi and seborrheic keratoses with a characteristic mutation pattern. Proc Nat Acac Sci (USA) 2007; 104:13450 [PubMed]
7. Happle R. Linear Cowden nevus: a new distinct epidermal nevus. Eur J Dermatol 2007; 17:133 [PubMed]
8. Caux F, et al. Segmental overgrowth, lipomatosis, arteriovenous malformation and epidermal nevus (SOLAMEN) syndrome is related to mosaic PTEN nullizygosity. Eur J Hum Genet 2007; 15: 767 [PubMed]
9. Richardson ES, et al. A novel mutation and large size polymorphism affecting the V2 domain of keratin 1 in an African-American family with severe, diffuse palmoplantar keratoderma of the icthyosis hystrix curth-macklin type. J Invest Dermatol 2006; 126:79 [PubMed]
10. Carlson, JA, et al. Epidermodysplasia verruciforms-associated and genital-mucosal high-risk human papillomavirus DNA are prevalent in nevus subaceous of Jedassohn. J Am Acad Dermatol 2008;59:279 [PubMed]
© 2010 Dermatology Online Journal