Successful treatment of plasma cell cheilitis with topical tacrolimus: Report of two cases
Published Web Location
https://doi.org/10.5070/D34rd1p1jsMain Content
Successful treatment of plasma cell cheilitis with topical tacrolimus: Report of two cases
Yuka Hanami MD, Yoshikazu Motoki MD, Toshiyuki Yamamoto MD
Dermatology Online Journal 17 (2): 6
Department of Dermatology, Fukushima Medical University, Fukushima, Japan. yuka-66@fmu.ac.jpAbstract
Plasma cell cheilitis is an uncommon chronic inflammatory dermatitis that presents with flat to slightly elevated erosive erythematous plaques. It is histologically characterized by plasma cell infiltrates into the mucosa. Other than the lip, genital areas are often involved, which is called plasma cell balanitis or vulvitis. Plasma cell cheilitis is sometimes resistant to conventional topical corticosteroid therapy. Other choices include oral griseofulvin, topical cyclosporine, and intralesional corticosteroid injection, all of which occasionally fail to produce satisfactory results. Recent reports show that topical calcineurin inhibitors are effective for plasma cell cheilitis, balanitis, and vulvitis. However, there are so far only 2 reports of plasma cell cheilitis successfully treated with topical pimecrolimus and tacrolimus. We present herein two cases of plasma cell cheilitis, in which topical tacrolimus showed beneficial effects, suggesting that this immunomodulatory agent is a promising option for plasma cell cheilitis.
Introduction
Plasma cell cheilitis is an uncommon chronic inflammatory dermatitis that presents with flat to slightly elevated erosive erythematous plaques. It is histologically characterized by plasma cell infiltrates into the mucosa. Other than the lip, genital areas are often involved, plasma cell balanitis or vulvitis. Plasma cell cheilitis is sometimes resistant to conventional topical corticosteroid therapy. Other choices include oral griseofulvin, topical cyclosporine, and intralesional corticosteroid injection [1, 2, 3], all of which occasionally fail to produce satisfactory results. Recent reports show that topical calcineurin inhibitors are effective for plasma cell cheilitis, balanitis, and also vulvitis [4-9]. However, there are so far only 2 reports of plasma cell cheilitis successfully treated with topical pimecrolimus and tacrolimus [8, 9]. We present herein two cases of plasma cell cheilitis in which topical tacrolimus showed significant benefit, suggesting that this immunomodulatory agent is a promising option for plasma cell cheilitis.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
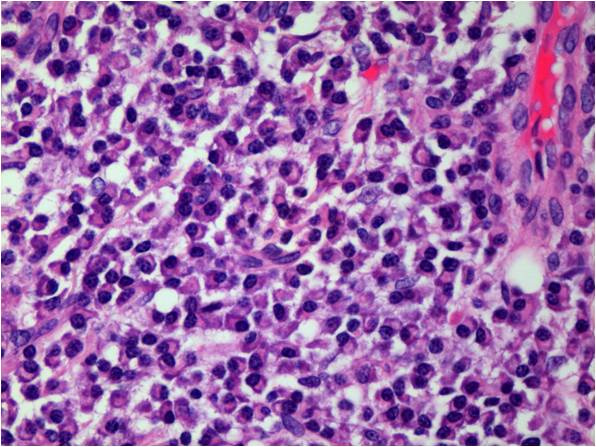
| Figure 1. Erythematous erosive plaques on the lower lip before treatment (Case 1) Figure 2. A biopsy specimen shows dense infiltrates composed of plasma cells | |
 |
| Figure 3 |
|---|
| Figure 3. Beneficial improvement after 1 month of topical tacrolimus therapy |
Case 1. A 66-year-old man was referred to our hospital, complaining of erythematous, erosive lesions on the lip for 3 months. He had been treated with various therapies such as topical corticosteroids, antibiotic ointment, and hydrocolloid dressings with no success. Physical examination showed erythematous erosive plaques on his lower lip (Figure 1). A biopsy specimen showed dense dermal infiltrates composed mainly of plasma cells (Figure 2). Results of immunohistochemical studies showed positive findings for IgG, κ, and λ. After providing informed consent, the patient was instructed to apply tacrolimus 0.1 percent ointment (Protopic®, Astellas Pharmaceutical Co. Ltd., Tokyo, Japan) twice daily. Great improvement was observed after 1 month of treatment (Figure 3).
Case 2. A 71-year-old man had erythematous, erosive lesions on the lip for 7 months. He had been treated with topical corticosteroids before he visited our hospital. Examination showed well-demarcated erythematous erosive plaques with crusts on his lower lip. A biopsy specimen showed dermal infiltrates that consisted mainly of plasma cells, which were immunoreactive for IgG, κ, and λ. The patient was instructed to apply tacrolimus 0.1 percent ointment twice daily and an almost complete response was observed after 1 month of treatment.
Discussion
Plasma cell cheilitis commonly affects the lip. In addition, buccal mucosa, palate, gingiva, tongue, epiglottis, and larynx can also be involved. Traumatic, genetic, hormonal, and autoimmune factors have been regarded as possible etiologic factors. Recently, topical calcineurin inhibitors have been shown to be effective for plasma cell cheilitis, balanitis, and vulvitis [4-9]. Calcineurin is a calcium-binding cytoplasmic protein that is involved in T-cell activation and proliferation. Immunomodulatory effects of calcineurin inhibitors include prevention of the dephosphorylation of the nuclear factor of activated T-cells (NFAT), which leads to the blocking of a cascade of gene transcription of inflammatory cytokines. Inhibitory effects on mast cells, Langerhans cells, T-cells, and eosinophils have been documented. By contrast, its mode of action for plasma cells is not known. Alternatively, from the viewpoint of site of application, tacrolimus is dramatically effective for mucous membrane lesions, such as those in orogenital areas. There are a number of reports in which topical tacrolimus was shown effective for oral and vulvovaginal lichen planus and lichen sclerosus on mucous membrane sites (lip, vulvar). Furthermore, topical tacrolimus has been beneficial for perianal ulcerating Crohn disease [10].
Although the precise mechanism of its action on plasma cell cheilitis is still unknown, complete remission was obtained in our cases by short courses of simple application of 0.1 percent topical tacrolimus twice daily, without any adverse effects. Neither of our patients complained of irritation, even when they applied tacrolimus ointment to the eroded lesions. After obtaining remission, the treatment has been continued intermittently when slight erythema appeared; neither of them have had recurrence or complication. Percutaneous absorption of topical tacrolimus is shown to be low because of its high molecular weight. On the contrary, unknown amounts of tacrolimus may be absorbed through injured mucous epithelium.
References
1. Tamaki K, Osada A, Tsukamoto K, Ohtake N, Furue M. Treatment of plasma cell cheilitis with griseofulvin. J Am Acad Dermatol 1994 May;30(5 Pt 1):789-90. [PubMed]2. Heinemann C, Fischer T, Barta U, et al. Plasma cell mucositis with oral and genital involvement-successful treatment with topical cyclosporine . J Eur Acad Dermatol Venereol 2006 Jul;20(6):739-40. [PubMed]
3. Tseng JT, Cheng CJ, Lee WR, et al. Plasma-cell cheilitis: successful treatment with intralesional injections of corticosteroids. Clin Exp Dermatol 2009 Mar;34(2):174-7. [PubMed]
4. Moreno-Arias GA, Camps-Fresneda A, et al. Plasma cell balanitis treated with tacrolimus 0.1%. Br J Dermatol. 2005 Dec;153(6):1204-6.[PubMed]
5. Hague J, Ilchyshyn A. Successful treatment of Zoon's balanitis with topical tacrolimus. Int J Dermatol. 2006 Oct;45(10):1251-2. No abstract available. [PubMed]
6. Roe E, Dalmau J, et al. Plasma cell balanitis of zoon treated with topical tacrolimus 0.1%: report of three cases. J Eur Acad Dermatol Venereol. 2007 Feb;21(2):284-5. No abstract available. [PubMed]
7. Virgili A, Mantovani L, et al. Tacrolimus 0.1% ointment: is it really effective in plasma cell vulvitis? Report of four cases. Dermatology. 2008;216(3):243-6. [PubMed]
8. Choi JW, Choi M, Cho KH. Successful treatment of plasma cell cheilitis with topical calcineurin inhibitors. J Dermatol. 2009 Dec;36(12):669-71. [PubMed]
9. Jin SP, Cho KH, Huh CH. Plasma cell cheilitis, successfully treated with topical 0.03% tacrolimus ointment. J Dermatolog Treat 2010 May;21(3):130-2. [PubMed]
10. Hart A, Plamondon S, Kamm MA. Topical tacrolimus in the treatment of perianal Crohn’s disease: exploratory randomized controlled trial. Inflamm Bowel Dis. 2007 Mar;13(3):245-53. [PubMed]
© 2011 Dermatology Online Journal