Inflammatory myofibroblastic tumor of the tongue: Report of an unusual case in a teenage patient
Published Web Location
https://doi.org/10.5070/D31q0631bmMain Content
Inflammatory myofibroblastic tumor of the tongue: Report of an unusual case in a teenage patient
Silvia Vanessa Lourenço1 DDS PhD, Paula Boggio2 MD, Marcello Menta Simonsen Nico2 MD
Dermatology Online Journal 18 (5): 6
1. Department of General Pathology, Dental School, University of São Paulo, Brazil2. Department of Dermatology, Medical School, University of São Paulo, Brazil
Abstract
Inflammatory myofibroblastic tumor is a rare and distinctive lesion composed of myofibroblastic cells accompanied by an inflammatory infiltration of plasma cells, lymphocytes, and eosinophils that mainly affects viscera and soft tissues of children and young adults. It clinically manifests as a mass with rapid development that may occur at almost any site of the body, but predominantly in the lungs or the upper respiratory tract. It rarely arises in the oral cavity with approximately 15 cases reported in that location. We describe a case of an inflammatory myofibroblastic tumor of the tongue, confirmed by both histopathologic and immunohistochemical analysis, occurring in a 14-year-old boy that spontaneously regressed after the surgical procedures for its diagnosis. Because of some aggressive clinical, histological, and radiological features, this lesion may be confused with a malignant tumor. Therefore, its correct recognition is important to avoid unnecessary extensive and radical therapeutic approaches.
Introduction
The term inflammatory myofibroblastic tumor (IMT), according to the classification of the World Health Organization established in 2002, has been applied to encompass a distinctive neoplasm composed of myofibroblastic cells accompanied by an inflammatory infiltration of plasma cells, lymphocytes, and eosinophils [1, 2].
Originally described in the lung by Brumm, in 1939, extrapulmonary IMT has also been reported at varied anatomic sites, mainly soft tissues and viscera [3, 4]. Head and neck lesions represent 14 percent to 18 percent of the extrapulmonary IMT cases; amongst these, oral lesions are very uncommon [5, 6, 7].
In the oral cavity, IMT consists of a rapidly growing tumor, which is histologically composed of fibrous and inflammatory tissue in a variety of histological patterns [5, 6, 7].
We report herein an unusual case of IMT of the tongue occurring in a male teenager.
Clinical case
 |  |
| Figure 1A | Figure 1B |
|---|---|
| Figures 1A and 1B. Clinical aspect of the inflammatory myofibroblastic tumor: Infiltrated mass on the dorsum of the tongue with a central ulceration. | |
A 14-year-old male presented with a 1-month history of a painful mass on the tongue. Oral examination revealed a firm, solitary, centrally ulcerated nodule on the dorsum of the tongue, measuring approximately 2 cm in diameter (Figures 1A and 1B). Remaining physical examination was unremarkable. He denied previous diseases and there was no history of preceding local trauma. Routine laboratory data presented no alterations or were within normal limits.
 |  |
| Figure 2A | Figure 2B |
|---|---|
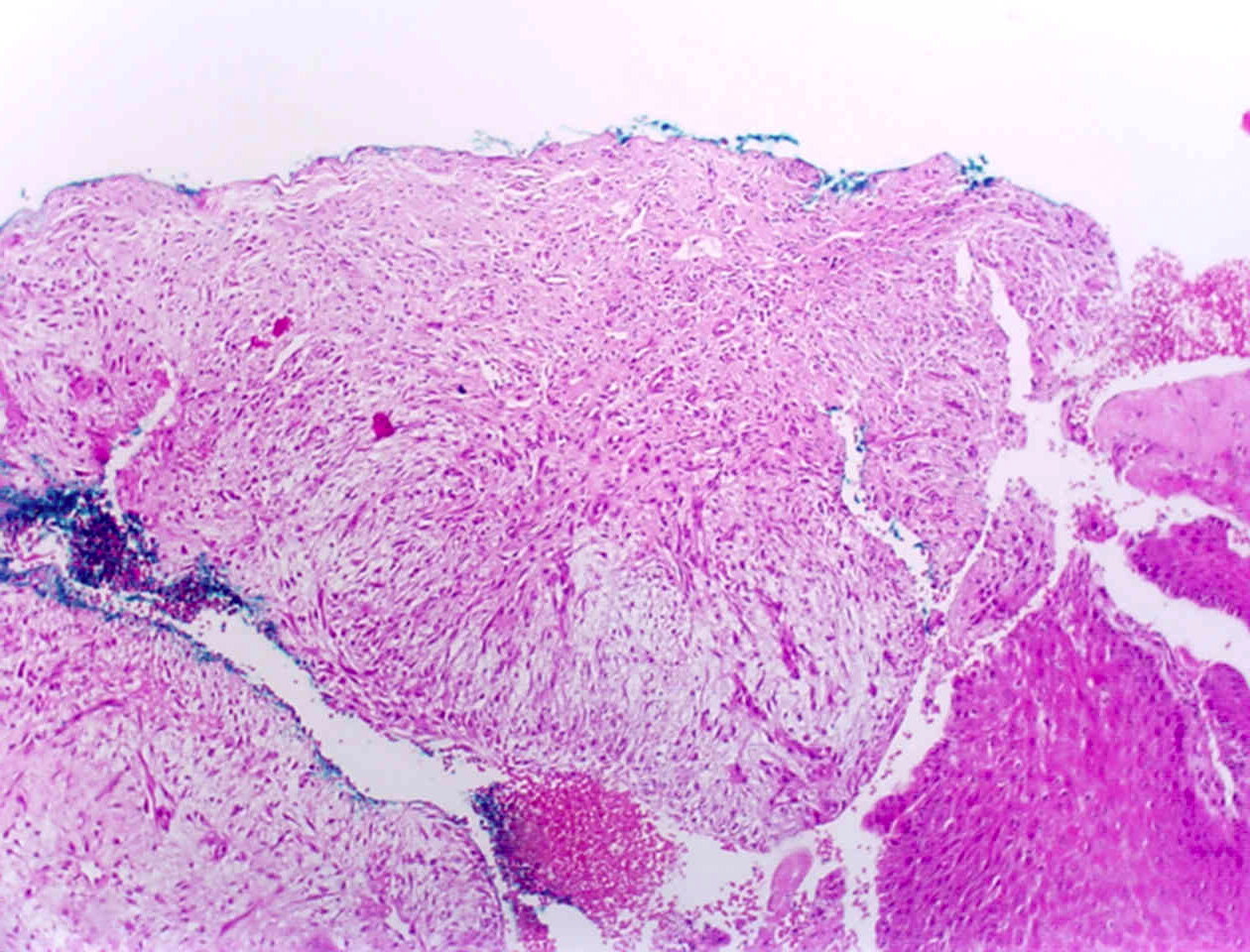
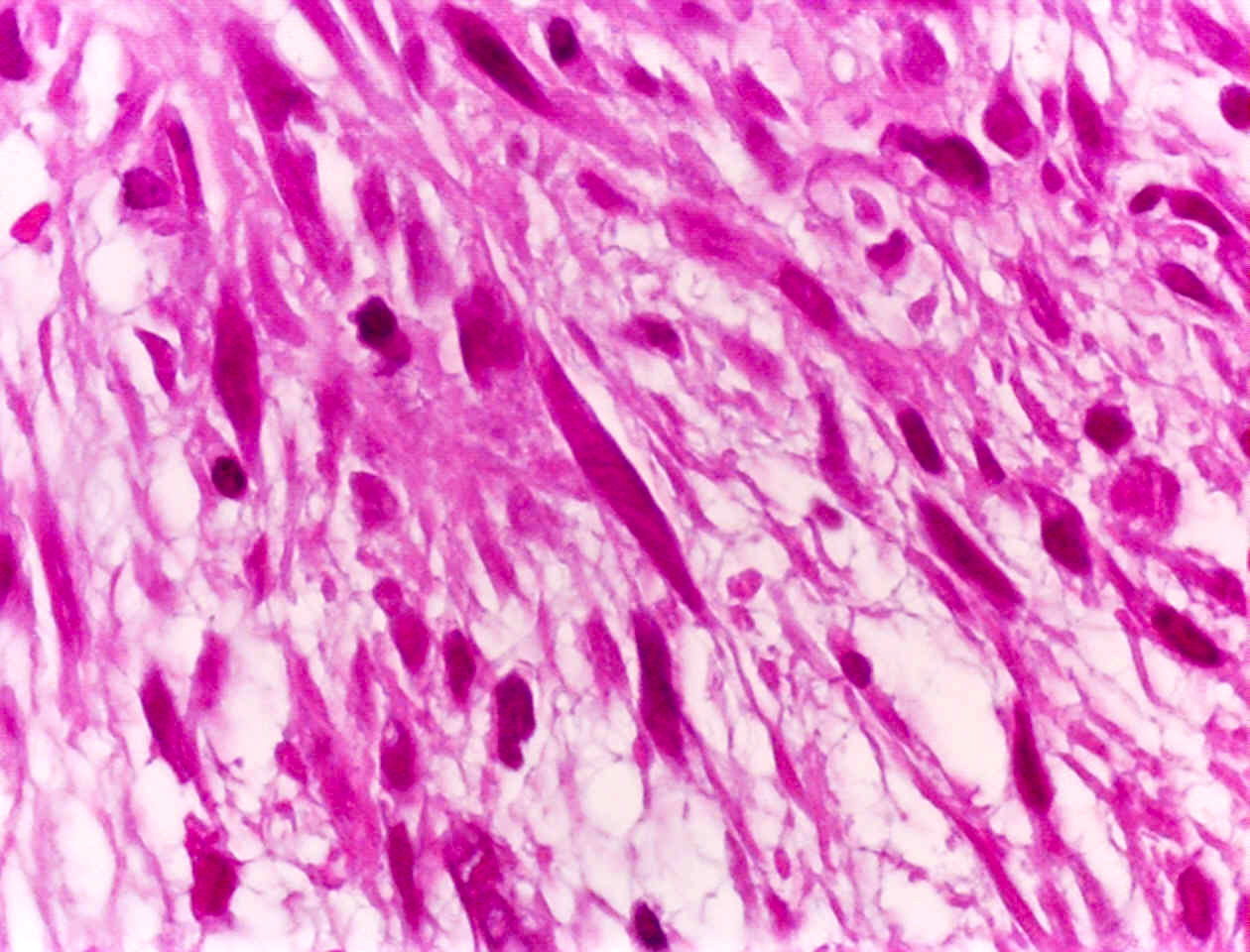
| Figure 2A. Lower magnification of the incisional biopsy shows spindle cell proliferation on a myxoid background, on the deeper
aspect of the lamina propria (H&E, x40). Figure 2B. Spindle cell proliferation permeated with inflammatory infiltrate in a myxoid background (H&E, x150). Figure 2C. Plump spindle cell and inflammatory infiltrate (H&E, x400). | |
 |
| Figure 2C |
|---|
An incisional biopsy was taken from the tumor and microscopic examination revealed a loosely arranged proliferation of plump spindle cells on a myxoid background, intermingled with lymphocytes and plasma cells, located in the deep lamina propria (Figures 2A to 2C). Special stains for microorganisms, including mycobacteria and fungi, were negative. Foreign bodies were also not found. Immunohistochemistry showed spindle cells positive for vimentin and smooth muscle actin.
The patient was lost to immediate follow-up, but returned 6 months after the initial biopsy and complete regression of the lesion could be observed. At present, 5 years after the diagnosis, he presents no recurrences.
Discussion
Inflammatory myofibroblastic tumor is a rare tumor constituted by a proliferation of myofibroblasts together with inflammatory cells intermingled within collagen fibers. Historically, this entity received several denominations, including plasma cell granuloma, inflammatory pseudotumor (IPT), and inflammatory myohistiocytic proliferation [2, 5, 8, 9].
Various pathogenic factors have been implicated in the etiology of IMT. However, its cause remains unclear. Trauma or chronic irritation can be the stimulus to an inflammatory response with reactive tissue proliferation and participation of myofibroblasts; in this sense several oral IMT have been preceded by mucosal trauma [10, 11]. Naitoh et al. suggest that IMT may be considered an IgG4-related autoimmune disease [12]. Many bacterial agents (more frequently M. avium intracellulare, Corynebacterium equi, Bacillus sphaerius, and Coxiella burnetti) and fungi have been associated with IMT [4]. Evidence of Epstein-Barr virus (EBV) infection has also been documented in most lesions arising in lymph nodes, spleen, and liver [5, 13, 14]. Recently, Human herpesvirus-8 has been reported as another possible etiologic agent [4, 15]. A careful history was performed in our patient and we could not find any apparent stimulus for the development of his tongue tumor.
The neoplastic nature of IMT has been largely debated. Whereas some authors believe it to be a reactive tumor and consider it analogous to inflammatory fibrosarcoma, others regard it as a low-grade malignancy or a lesion with uncertain malignant biology, particularly those occurring in the liver and the spleen [3, 16, 17, 18].
Although the term IMT has been used synonymously with IPT in the past, recently IMT has been recognized as an intermediate neoplasm of myofibroblastic spindle cells associated with inflammatory infiltrates, that may present malignant features [2, 8, 9, 19]. IPT continues to be considered as a lesion of reactive nature. By cytogenetic studies some cases of IMT have demonstrated several clonal chromosomal aberrations involving 2p23, with alterations occurring in or near the ALK (anaplastic lymphoma kinase) gene, supporting the concept of a true neoplasm [2, 8]. The resultant ALK protein overexpression in the myofibroblastic component of those tumors can be demonstrated by immunohistochemistry [2, 8, 19, 20].
Nonetheless the controversy continues and we must remember that papers reporting IPT and IMT include a heterogeneous group of neoplastic entities that appear histologically similar but mainly differ in biological behavior [19]. For the true neoplasms the denomination IMT would be desirable, whereas the non-neoplasic lesions should be considered IPT or plasma cell granuloma.
Inflammatory myofibroblastic tumor can occur at any age, but mainly affects the lungs of children and young adults [3, 4, 21]. Its occurrence in the oral cavity is extremely rare. In a recent review of the literature, Brooks et al. found 15 cases reported of IMT in the various oral sites [5]. The cheek and the mandible seem to be the areas of predilection [20]. In a further search we have only encountered 4 cases located on the tongue [14, 21, 22, 23], as the case herein presented.
This tumor may be completely asymptomatic or may manifest with fever of unknown cause in childhood. Sometimes, obstructive or compressive symptoms, depending upon the viscera affected, may be accompanied by systemic symptoms such as fever, weight loss, and malaise [4].
Clinically, oral IMT appears more commonly as a well-circumscribed solitary nodule or as a painless and firm swelling, both of relative short duration. Some cases have presented with exuberant fibrosis and contraction of deeper tissues [5]. Unlike the visceral counterpart, oral lesions do not produce significant systemic symptoms [20].
Histologically, IMT is composed of a myofibroblastic cellular population in a variably collagenous stroma admixed with inflammatory cells, chiefly lymphocytes and plasma cells [1, 5]. Depending on the relative proportion of each component, myofibroblastic and inflammatory, the diagnosis of IMT sometimes may be difficult, with a spectrum that ranges from lesions indistinguishable from a reactive process to those that appear sarcomatous [8]. Three basic histologic patterns can be recognized: a) a myxoid/vascular pattern with spindle or stellate myofibroblasts in an abundant myxoid stroma with an inflammatory component resembling granulation tissue or nodular fasciitis; b) compact spindle cells that may adopt a storiform pattern intermingled with inflammatory cells resembling fibrous histiocytoma or fibromatoses; and c) dense plate-like collagen with low cell density and rare inflammatory cell stroma, resembling a desmoid or a scar [9, 10]. The lack of necrosis, the cytologic monotony of the proliferating cells, and the lack of atypical mitotic features suggest the benign nature of IMT. Immunohistochemistry is important for the final diagnosis and the spindle cells are usually positive for vimentin, desmin, muscle-specific actin, and smooth-muscle-actin (SMA) [3, 5]. They also frequently show positive staining with antibodies against ALK-1 protein [19]. The tongue lesion reported herein presented with the myxoid/vascular histologic pattern and the spindle cells were markedly positively for vimentin and SMA; ALK-1 and ALK gene rearrangement could not be performed.
It is important to remember that IMT can sometimes be a clinical and radiological simulator of malignancy showing features of significant bony destruction [5]. It is therefore essential to establish a correct histopathologic diagnosis in order to avoid aggressive unnecessary treatment.
Patients with IMT with visceral involvement often have non-specific laboratory abnormalities such as anemia, leukocytosis, thrombocytosis, elevated erythrosedimentation rate, and hypergammablobulinemia [4]. That was not the case in our patient who presented in a good general state and showed a normal routine laboratory evaluation.
In all locations, the differential diagnosis should include primary or metastatic neoplasms. The list is extensive, but the main entities to be clinically considered when oral, based on their frequency of occurrence, include: squamous cell carcinoma, chancre of primary syphilis, nodular fasciitis, myoepitheliomas, and malignant sarcomas, amongst others [5]. The presence of an oral tumor with rapid growth and spontaneous regression after biopsy, associated with the morphology and arrangement of the myofibroblastic cells (confirmed immunohistochemically) and the dense inflammatory component, were the principal features that led us to final diagnosis of IMT. However, because of the impossibility of evaluating ALK1 staining as well as ALK gene rearrangement, it could be debated that this case should be labeled as IPT.
Inflammatory myofibroblastic tumor of the oral cavity has been treated as a benign lesion with satisfactory results [5, 24]. Simple excision of the tumor has proved to be effective in controlling these, without recurrences when complete. Other treatment modalities described in the literature are steroid therapy, curettage, radiotherapy, and chemotherapy. Long-term follow-up is mandatory in IMT, because some cases have behaved as true malignant tumors. Yet, rare cases may undergo spontaneous regression as seen in the present report [3, 5, 25, 26].
Some investigators also mention that in their experience, head and neck IMT, especially intra-oral forms, have a better prognosis than lesions elsewhere [23].
The present case reports a circumscribed tumor of the tongue consisting of a proliferation of fibro-inflammatory nature, diagnosed as IMT, in a teenage boy that resolved spontaneously and has not recurred. An argument could also be made for designating this as IPT in this patient. Clinico-pathologic correlation is required in order to establish this diagnosis. The current controversy between the diagnosis of IMT and IPT strongly suggests that further studies with a greater number of cases are needed to correctly classify these oral lesions.
References
1. Coffin CM, Fletcher JA. Inflammatory myofibroblastic tumor. In: Fletcher CDM, Unni KK, Mertens F, eds. World Health Organization Classification of Tumours. Pathology and Genetics of tumors of soft tissue and bone. Lyon (France): IARC Press; 2002. pp. 91-3.2. Ishihara M, Izumoto S, Iwatsuki K, Yoshimine T. Immunohistochemical study of multiple inflammatory pseudotumors with both brain and spinal cord involvement. Neurol Med Chir 2010; 50(3): 246-50. [PubMed]
3. Coffin CM, Watterson J, Priest JR, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor). A clinicopathologic and immunohistochemical study of 84 cases. Am J Surg Pathol 1995; 19(8): 859-72. [PubMed]
4. Lisarbe MO, JH, García ER, Castiella TM, Sagaseta de Ilúrdoz Uranga María M, Garicano JM. Paediatric myofibroblastic tumours. A presentation of three cases. An Pediatr (Barc) 2009; 71(4): 331-35. [PubMed]
5. Brooks JK, Nikitakis NG, Frankel BF, Papadimitriou JC, Sauk JJ. Oral inflammatory myofibroblastic tumor demonstrating ALK, p53, MDM2, CDK4, pRb and Ki-67 immunoreactivity in an elderly patient. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; 99(6): 716-26. [PubMed]
6. Monteil RA, Saint-Paul MC, Hofman P, Jehl-Pietri C, Michiels JF, Raspaldo H. Oral inflammatory pseudotumour: immunohistochemical investigation of a case involving the submandibular gland and review of the literature. Oral Oncol 1997; 33(3): 215-9. [PubMed]
7. Arber DA, Kamel OW, van de Rijn M, Davis RE, Medeiros LJ, Jaffe ES, Weiss LM. Frequent presence of the Epstein-Barr virus in inflammatory pseudotumor. Hum Pathol 1995; 26(10); 1093-8. [PubMed]
8. Griffin CA, Hawkins AL, Dvorak C, Henkle C, Ellingham T, Perlman EJ. Recurrent involvement of 2p23 in inflammatory myofibroblastic tumors. Cancer Res. 1999; 59(12): 2776-80. [PubMed]
9. Zhang Y, Dong Z, Zhi X, Liu L, Hu M. Inflammatory myofibroblastic tumor in lung with osteopulmonary arthropathy. Chin Med J 2009; 122(24): 3094-6. [PubMed]
10. Ide F, Shimoyama T, Horie N. Sclerosing inflammatory myofibroblastic tumour of the tongue: an immunohistochemical and ultrastructural study. Oral Oncol 2000; 36(3): 300-4. [PubMed]
11. Zellers RA, Bicket WJ, Parker MG. Post traumatic spindle cell nodule of the buccal mucosa. Report of a case. Oral Surg Oral Med Oral Pathol 1992; 74(2): 212-5. [PubMed]
12. Naitoh I, Nakazawa T, Ohara H, Ando T, Hayashi K, Tanaka H, et al. IgG4-related hepatic inflammatory pseudotumor with sclerosing cholangitis: a case report and review of the literature. Cases J 2009; 11(2): 7029. [PubMed]
13. Arber DA, Weiss LM, Chang KL. Detection of Epstein-Barr virus in inflammatory pseudotumor. Semin Diagn Pathol 1998; 15(2): 155-61. [PubMed]
14. Lewis JT, Gaffney RL, Casey MB, Farrell MA, Morice WG, Macon WR. Inflammatory pseudotumor of the spleen associated with a clonal Epstein-Barr virus genome. Case report and review of the literature. Am J Clin Pathol 2003; 120(1): 56-61. [PubMed]
15. Gómez-Román JJ, Sánchez-Velasco P, Ocejo-Vinyals G, Hernández-Nieto E, Leyva-Cobián F, Val-Bernal JF. Human herpesvirus-8 genes are expressed in pulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor). Am J Surg Pathol 2001; 25(5): 624-9. [PubMed]
16. Su LD, Atayde-Perez A, Sheldon S, Fletcher JA, Weiss SW. Inflammatory myofibroblastic tumor: cytogenetic evidence supporting clonal origin. Mod Pathol 1998; 11(4): 364-8. [PubMed]
17. Cheuk W, Chan JK, Shek TW, Chang JH, Tsou MH, Yuen NW, et al. Inflammatory pseudotumor-like follicular dendritic cell tumor. A distinctive low-grade malignant intra-abdominal neoplasm with consistent Epstein-Barr virus association. Am J Surg Pathol 2001; 25(6): 721-31. [PubMed]
18. Rosenbaum L, Houman Fekrazad M, Rabinowitz I, Vasef MA. Epstein-Barr virus-associated inflammatory pseudotumor of the spleen: report of two cases and review of the literature. J Hematopathol 2009; 2: 127-31. [PubMed]
19. Swain RS, Tihan T, Horvai AE, Di Vizio D, Loda M, Burger PC, et al. Inflammatory myofibroblastic tumor of the central nervous system and its relationship to inflammatory pseudotumor. Hum Pathol 2008; 39(3): 410-9. [PubMed]
20. Shek AW, Wu PC, Samman N. Inflammatory pseudotumor of the mouth and maxilla. J Clin Pathol 1996; 49(2): 164-7. [PubMed]
21. Soares J, Nunes JF, Sacadura J. Plasma cell granuloma of the tongue. Report of a case. Histol Histopathol 1987: 2(2): 199-201. [PubMed]
22. Gleizal A, Ranchere-Vince D, Abou-Chebel N, Nimeskern N, Béziat JL. Inflammatory myofibroblastic pseudotumor of the tongue. Rev Stomatol Chir Maxillofac 2005; 106(5): 304-7. [PubMed]
23. Pankaj C, Uma C. How to manage oral inflammatory myofibrobalstic tumor (inflammatory pseudotumor)? Oral Dis 2001; 7(5): 315-6. [PubMed]
24. Meis-Kindblom JM, Kjellström C, Kindblom LG. Inflammatory fibrosarcoma: update, reappraisal, and perspective on its place in the spectrum of inflammatory myofibroblastic tumors. Semin Diagn Pathol 1998; 15(2): 133-43. [PubMed]
25. Thompson RJ, Barrett AM, Dildey P. Congenital multifocal inflammatory pseudotumor: a case report. J Pediatr Surg 2003; 38(10): E17-9. [PubMed]
26. Biecker E, Zimmermann A, Dufour JF. Spontaneous regression of an inflammatory pseudotumor of the liver. Z Grastroenterol 2003; 41(10): 991-4. [PubMed]
© 2012 Dermatology Online Journal