Keratosis follicularis
Published Web Location
https://doi.org/10.5070/D371v042s0Main Content
Keratosis follicularis
Meredith K Kosann MD
Dermatology Online Journal 9(4): 35
From the Ronald O. Perelman Department of Dermatology, New York University
Abstract
Keratosis follicularis is a genetic disorder that is inherited in an autosomal dominant pattern. Physical examination classically shows keratotic papules that are distributed mostly on the so-called "seborrheic" areas of the body. Nail involvement is not uncommon and is characterized by V-shaped nicking at the distal aspect of the nail bed, longitudinal red and white alternating bands, and subungual hyperkeratosis. Mucosal membrane involvement may occur as white papules on the buccal mucosae, palate, and gingiva with a cobblestone appearance. The mutation has been traced to chromosome 12, where a spectrum of mutations within the ATP2A2 gene encode the calcium ATPase of the sarco/endoplasmic reticulum (SERCA2).
Clinical summary
History.—A 51-year-old man had a 37-year history of a dermatosis involving the face, trunk, extremities, and nails. When the patient presented to Bellevue Hospital Medical Center, he complained of pruritus and foul odor as well as ulcers on the lower extremities. The patient noted that his grandmother had a similar skin disease, although it was not so severe as the patient's condition. He noted improvement after the initiation of oral retinoids.
Physical examination.—Crusted, scaly, keratotic, erythematous papules and plaques extended over the extensor surfaces of the upper extremities, back, chest, and inguinal folds, with an associated malodor, erosions, excoriations, and honey-yellow crusts. Flat-topped papules were evident on the dorsa of the hands, and slightly scaly papules were present on the volar surfaces of the palms. The nails had V-shaped nicking and several erythematous linear bands. Mucosal surfaces were clear.

|

|
| Figure 1 | Figure 2 |
|---|
|
| Figure 3 |
|---|
Laboratory data.—The white cell count was 11.4 x 109/L, hemoglobin 14.2 g/dL, and the platelet count 234 x 109/L. Basic metabolic profile and hepatic function tests were normal.
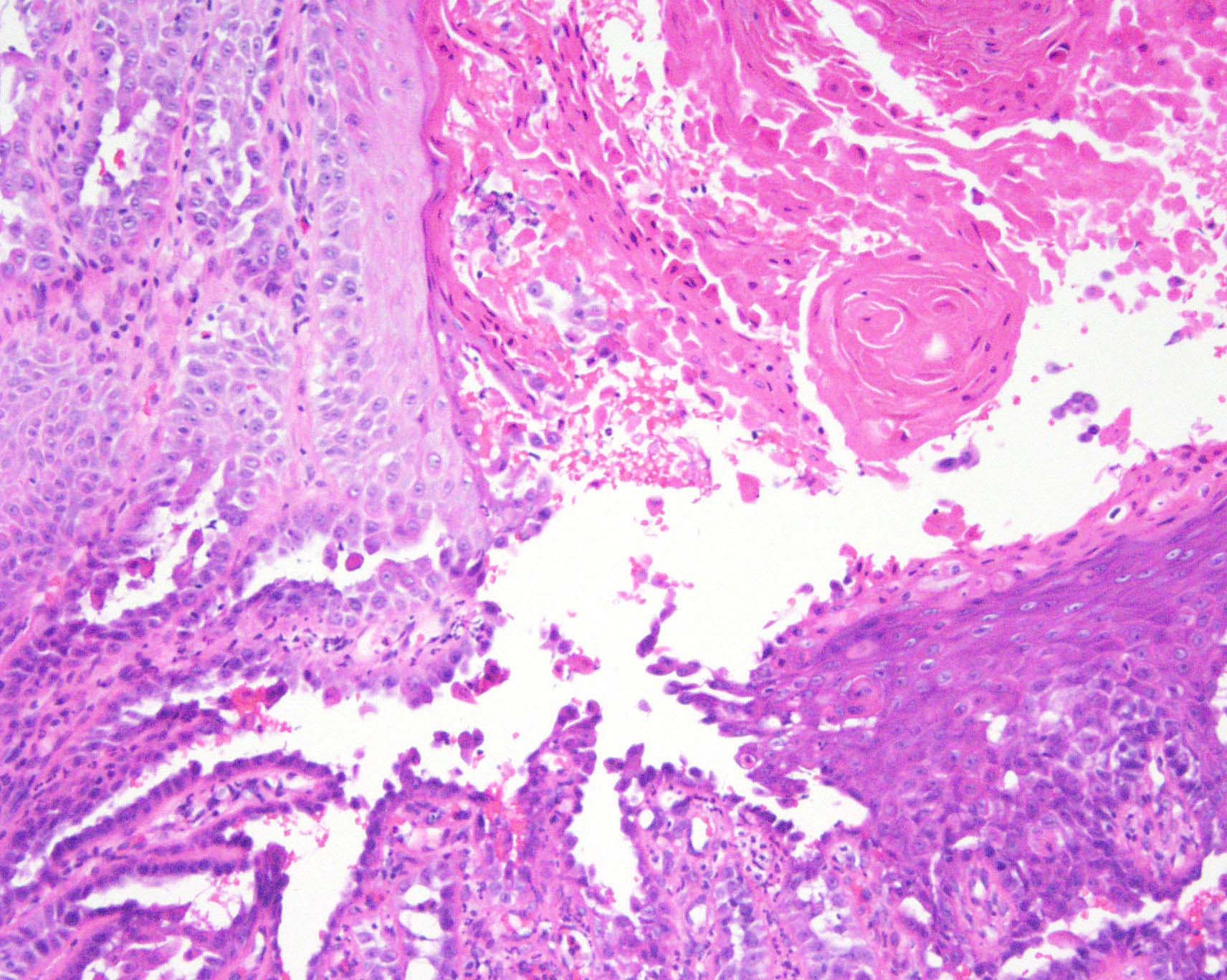
Histopathology.—There is a hyperplastic epidermis with suprabasilar acantholysis, dyskeratosis, and a column of parakeratosis.
Diagnosis.—Keratosis follicularis.
Comment
Keratosis follicularis (Darier-White disease) is a genetic disorder of abnormal keratinization. It is characterized clinically by scaly, warty, crusted papules distributed mostly on the seborrheic areas of the body. Nail involvement is characterized by V-shaped nicking at the distal aspect of the nail bed, longitudinal red and white alternating bands, and subungual hyperkeratosis. Mucosal membrane involvement may occur as white papules on the buccal mucosae, palate, and gingiva with a cobblestone appearance.
The disorder is a relatively common genodermatosis and affects approximately 1 in 36,000 individuals. It is characterized by late age of onset and typically presents in the first or second decade. The condition may be exacerbated by ultraviolet light exposure, particularly ultraviolet B, as well as by heat, humidity, and friction. The inheritance pattern is autosomal dominant, and the mutation has been traced to chromosome 12. A spectrum of mutations has been isolated within the ATP2A2 gene encoding the calcium ATPase of the sarco/endoplasmic reticulum (SERCA2) [1].
Oral retinoids have been reported to be effective treatments of keratosis follicularis. Topical tazarotene, [2] topical isotretinoin, [3] and topical adapalene [4] have been shown to be effective.
Oral contraceptives were reported to be effective in the treatment of one patient, who had perimenstrual flares of her disease [5]. Surgical treatment includes dermabrasion, carbon dioxide laser, and the erbium YAG laser [6]. In addition, use of topical sunscreens and ascorbic acid have been shown to be effective in the prevention of disease flares [7].
References
1. Sakuntabhai A, et al. Mutations in ATP2A2, encoding a Ca2+ pump, cause Darier disease. Nat Genet 21:271 1999.2. Enk Oster-Schmidt C. The treatment of Darier's disease with topical tazarotene. Br J Dermatol 141:603, 1999.
3. McKenna KE, et al. Treatment of unilateral Darier's disease with topical isotretinoin. Clin Exp Dermatol 24:425, 1999.
4. English JC III, et al. Effective treatment of localized Darier's disease with adapalene 0.1% gel. Cutis 63:227, 1999.
5. Oostenbrink JH, et al. Oral contraceptives in the treatment of Darier-White disease: A case report and review of the literature. Clin Exp Dermatol 21:442, 1996.
6. Beier C, Kaufmann R. Efficacy of erbium:YAG laser ablation in Darier disease and Hailey-Hailey disease. Arch Dermatol 135:423, 1999.
7. Heo EP, et al. Induction of Darier's disease by repeated irradiation by ultraviolet B: Protection by sunscreen and topical ascorbic acid. J Dermatol 29:455, 2002.
© 2003 Dermatology Online Journal