Collision Tumor: Importance of the new auxiliary tools for diagnosis (An illustrative case report)
Published Web Location
https://doi.org/10.5070/D331j5v69xMain Content
Letter: Collision Tumor: Importance of the new auxiliary tools for diagnosis (An illustrative case report)
Nuno Menezes MD, Guedes Rita, Leite Inês, Varela Paulo, Baptista Armando
Dermatology Online Journal 17 (7): 12
Abstract
Collision tumor is a term used to refer to the association of various types of tumors in time and space. Despite most of them not being clinically relevant, sometimes there is a union between a benign lesion and a malignant one. The clinical diagnosis in these cases is usually extremely difficult, particularly if one of the lesions is pigmented. Dermoscopy and confocal microscopy are noninvasive diagnostic methods that make possible the visualization of morphologic structures not visible to the naked eye, thus making diagnosis of these lesions possible. Here we describe a case in which the corrected diagnosis of a collision between a seborrheic keratosis and a basal cell carcinoma was only possible by means of confocal microscopy.
Introduction
The term collision tumor designates lesions in which two or more distinctive neoplasms arise together. Some authors consider the term collision tumor invalid because it implies that an accidental association has occurred thus eliminating the possibility of a relationship between the neoplasms. Therefore compound tumor would be a more appropriate term for these lesions [1]. The clinical accuracy of the naked eye to diagnose these lesions is limited and there are some reports in the literature that establishes the aid of dermoscopy for the diagnosis [2, 3, 4]. Confocal microscopy is an in vivo technique that allows a horizontal visualization of the lesions, thus bringing a new dimension to diagnosis. With this technique a horizontal visualization of the epidermis, the dermal-epidermal junction and the superficial dermis is achieved. The confocal microscopy criteria have been defined for pigmented lesions [5]. We describe the clinical, dermoscopic, and confocal microscopy characteristics of a compound tumor for which only the usage of confocal microscopy allowed the correct diagnosis to be made prior to biopsy.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
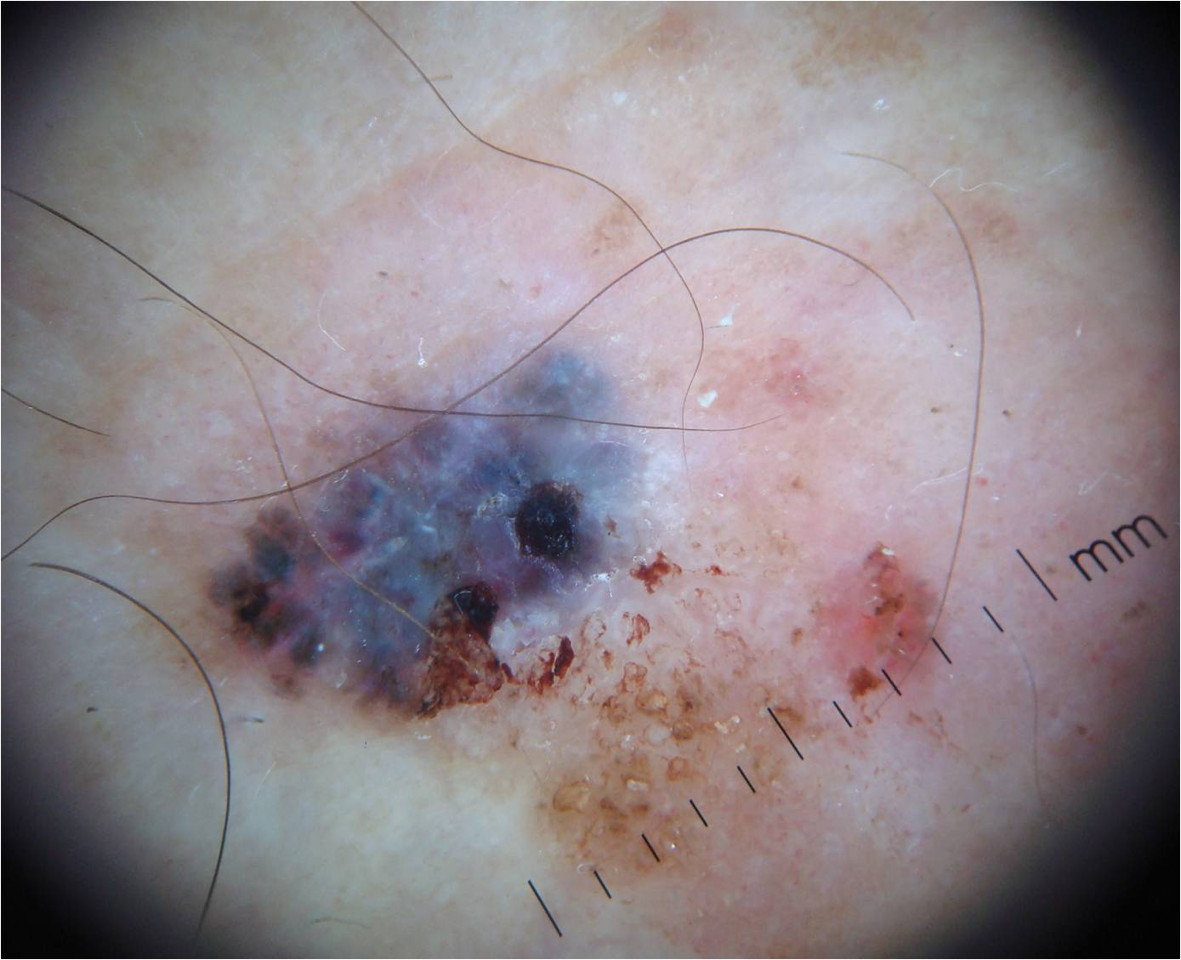
| Figure 1. Brown pigmented patch 4 cm in diameter with a dark round eccentric area Figure 2. Image with features of seborrheic keratosis with comedo-like openings, sharp border demarcation, and hairpin vessels; basal cell carcinoma with ulceration and maple-leaf like areas; and melanoma with the presence of a bluish-white veil and irregular linear vessels | |
A 64-year-old woman, with a long history of a brown asymptomatic patch located on the left lower limb, noticed a black papule starting to grow in that location 6 months previously, with a slow but constant increase in size. Clinical examination revealed a brown pigmented lesion, 4 cm in diameter, with a dark round area in an eccentric localization (Figure 1). Dermoscopy (DermLite Pro HR) revealed the criteria of three different lesion types. Seborrheic keratosis with comedo-like openings, sharp border demarcation, and hairpin vessels; basal cell carcinoma with ulceration and maple-leaf like areas; and melanoma with the presence of a bluish-white veil and irregular linear vessels (Figures 2 and 3).
 |  |
| Figure 3 | Figure 4 |
|---|---|
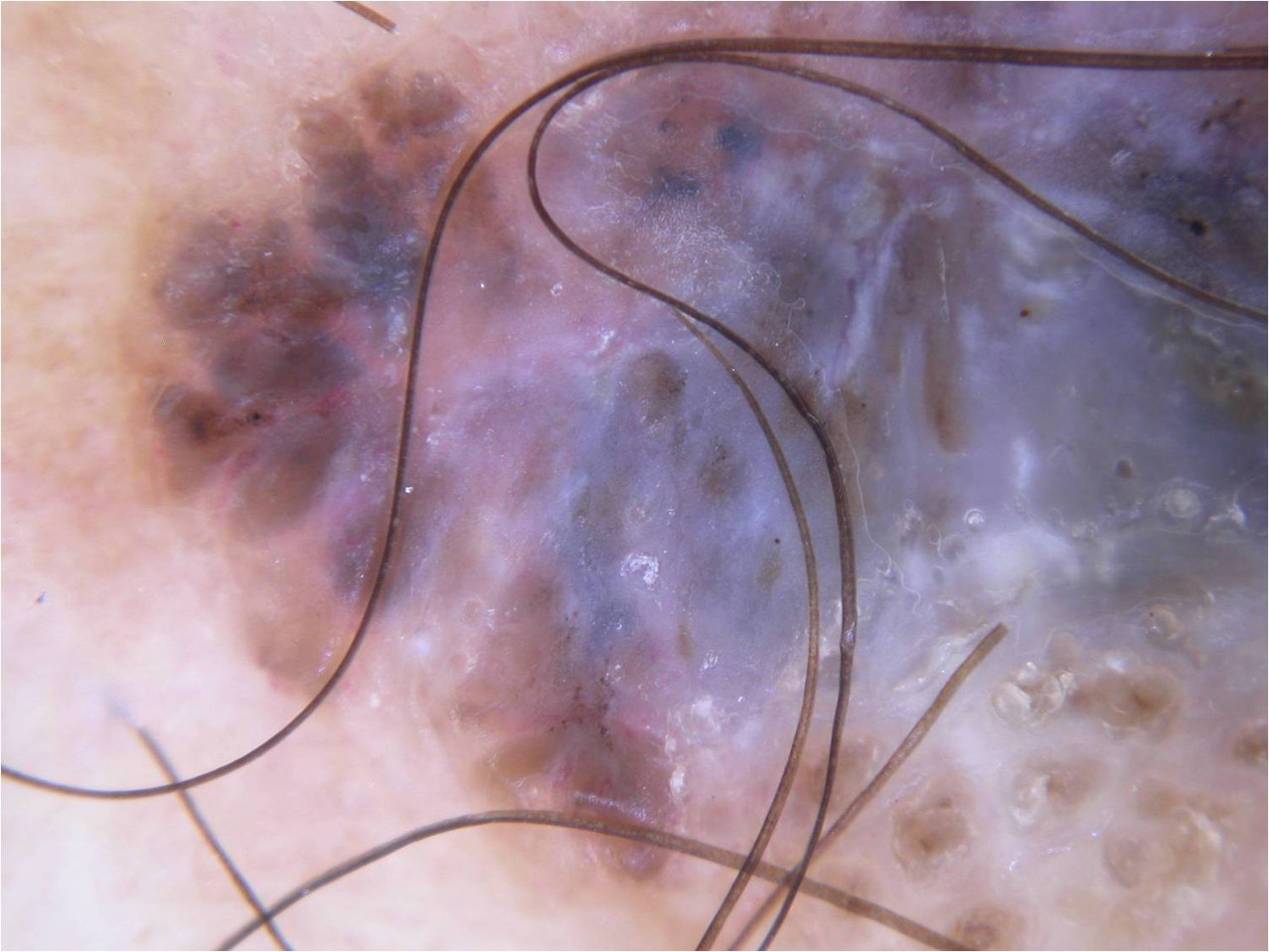
| Figure 3. Image with features of seborrheic keratosis with comedo-like openings, sharp border demarcation, and hairpin vessels;
basal cell carcinoma with ulceration and maple-leaf like areas; and melanoma with the presence of a bluish-white veil and
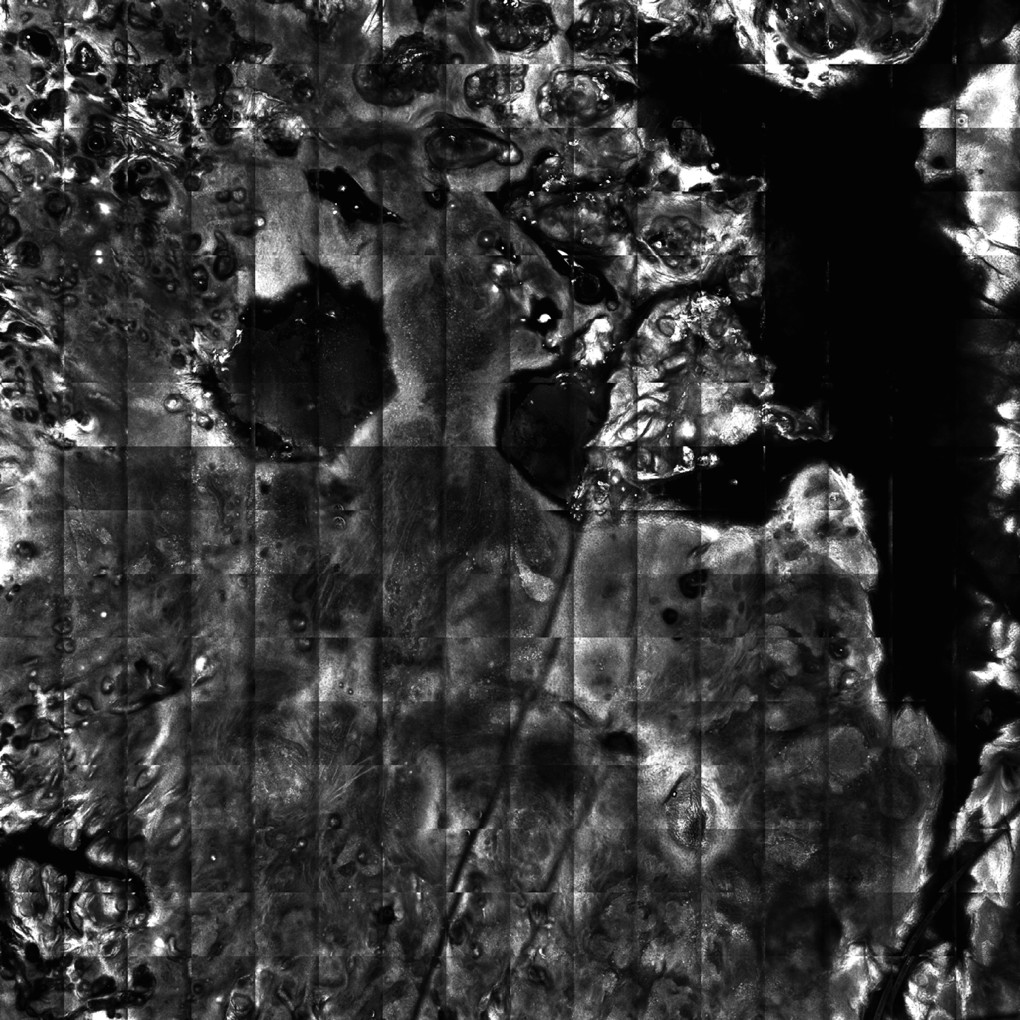
irregular linear vessels Figure 4. Mosaic at the level of dermo-epidermal junction showing the presence of tumor islands, cleft-like dark spaces suggestive of basal cell carcinoma. Areas with keratin-filled invaginations as well as bulbous projections suggestive for a seborrheic keratosis | |
 |
| Figure 5 |
|---|
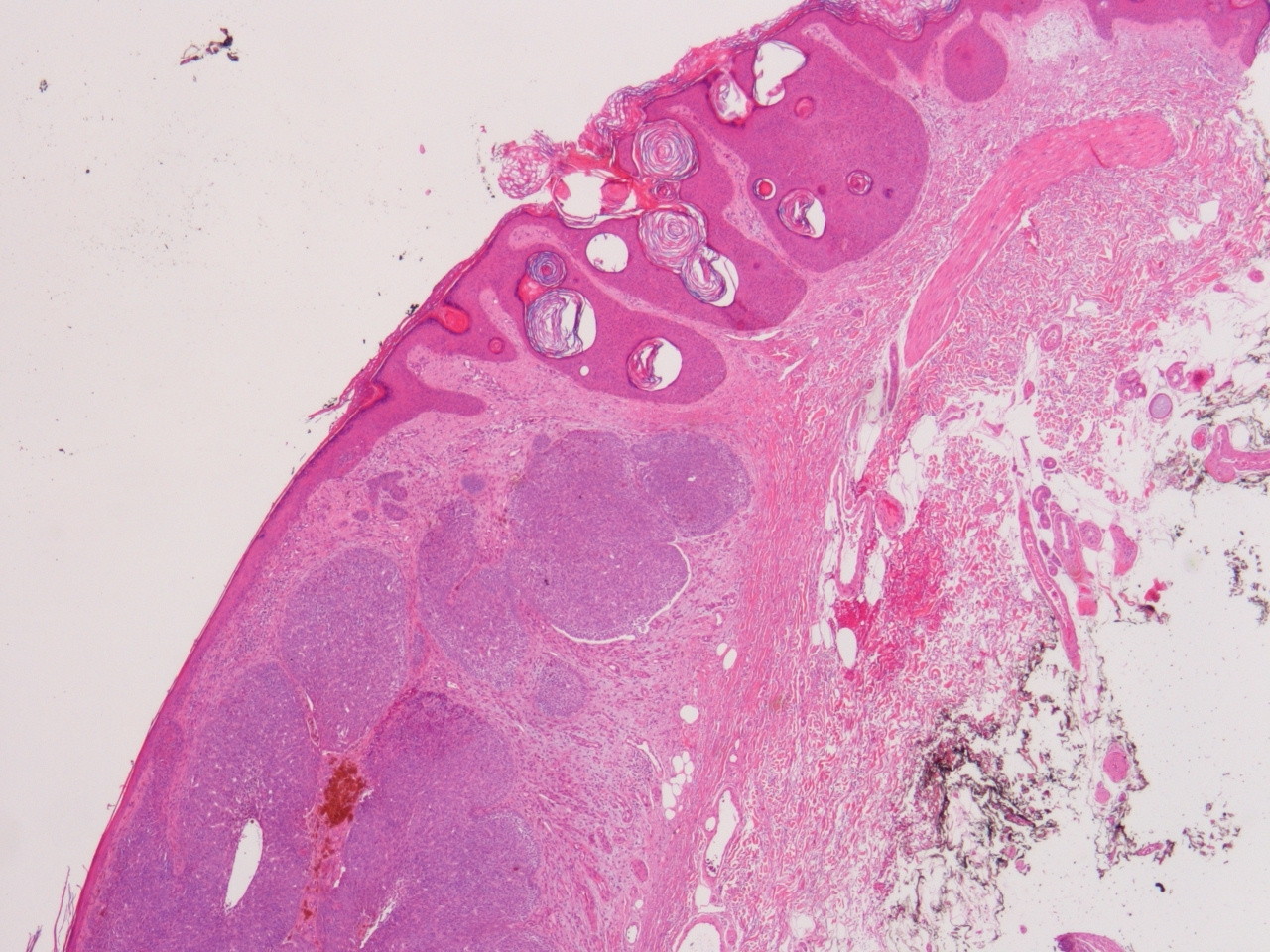
| Figure 5. Histological image of the lesion with features of basal cell carcinoma and seborrheic keratosis |
On confocal microscopy the mosaic at the level of dermo-epidermal junction showed the presence of tumor islands, cleft-like dark spaces suggestive for basal cell carcinoma. In addition, areas with keratin-filled invaginations as well as bulbous projections were suggestive of a seborrheic keratosis. There were no criteria for melanoma (Figure 4). This allowed us to propose the diagnosis of a compound tumor of seborrheic keratosis associated with basal cell carcinoma that was confirmed by histology (Figure 5).
Discussion
In this report we want to emphasize the importance of auxiliary means of diagnosis in the correct evaluation of pigmented lesions. This report also shows that confocal microscopy allows a more comprehensive evaluation of the lesions than dermoscopy. On dermoscopy, a diagnosis of a collision tumor with a melanoma associated would have been made. This fact would be excluded by confocal microscopy.
Although seborrheic keraosis is the most common cutaneous neoplasm, it is surprising that its coexistence with other cutaneous neoplasms is so rarely reported. This observation has led some researchers to consider this occurrence as a mere coincidence. According to Ferrara et al. this argument is biased by at least two main factors. First, the progressive growth of an aggressive neoplasm might entirely destroy an associated seborrheic keratosis. Second, a residual seborrheic keratosis might be easily overlooked on microscopic examination when limited to a few intraepidermal nests. For these reasons, the coexistence of seborrheic keratosis with other cutaneous neoplasms might be underdiagnosed [6].
The development of basal cell carcinoma in association with a seborrheic keratosis was first recognized by Sibley as early as 1932. Since then, this association has been rarely described (eight of 40,000 cases or 43 of 85,000 cases) [1].
Two different hypotheses have been proposed to explain the relationship between these two lesions. First, a pathogenic relationship may exist because both tumors arise from pluripotential cells of either the basal layer of the epidermis or the hair follicle epithelium. On the other hand, this association could represent simply the presence of two common lesions juxtaposed by coincidence [1, 7]. In our case, because the basal cell is on the middle of a seborrheic keratosis, it would be probably the case of the first hypothesis.
There are well defined criteria for dermoscopic diagnosis of these two lesions and confocal criteria are starting to be defined as well. In the future and with the help of technology more cases will be clinical delineated [8, 9, 10].
References
1. P Zaballos, A Llambrich, S Puig, J Malvehy. Dermoscopy is useful for the recognition of benign-malignant compound tumours. British Journal of Dermatology 2005 153, 653-656. [PubMed]2. I Fernández-Canedo, N Blázquez, M de Troya, T Pérez-Salguerob. Collision Tumor Detected by Dermoscopy. Actas Dermosifiliogr. 2009;100:615-34. [PubMed]
3. V de Giorgi, D Massi, S Sestini, B Alfaioli, G Carelli, P Carli. Cutaneous collision tumour (melanocytic naevus, basal cell carcinoma, seborrhoeic keratosis): a clinical, dermoscopic and pathological case report. Br J Dermatol. 2005 Apr;152(4):787-90. [PubMed]
4. A J Birnie, S Varma. A dermatoscopically diagnosed collision tumour: malignant melanoma arising within a seborrhoeic Keratosis. Clinical and Experimental Dermatology, 33, 512-513. [PubMed]
5. Rajadhyaksha M, Grossman M, Esterowitz D, Webb RH, Anderson RR. In vivo confocal scanning laser microscopy of human skin: melanin provides strong contrast. J Invest Dermatol 104:946-52. [PubMed]
6. G Ferrara, I Zalaudek, H Cabo, HP Soyer, G Argenziano. Collision of basal cell carcinoma with seborrhoeic keratosis: a dermoscopic aid to histopathology? Clinical and Experimental Dermatology, 30, 586-587. [PubMed]
7. Rao BK, Freeman RG, Poulos EG et al. The relationship between basal cell epithelioma and seborrheic keratosis. J Dermatol Surg Oncol 1994; 20:761-4. [PubMed]
8. Braun RP, Rabinovitz HS, Oliviero M, Kopf AW, Saurat JH. Dermoscopy of pigmented skin lesions. J Am Acad Dermatol 2005;52:109-21. [PubMed]
9. Agero ALC, Busam KJ, Benvenuto-Andrade C, Scope A, Gill M, Marghoob AA, Gonzalez S, Halpern AC. Reflectance confocal microscopy of pigmented basal cell carcinoma. J Am Acad Dermatol 2006;54:638-43. [PubMed]
10. Segura S, Puig S, Carrera C, Palou J, Malvehy J. Development of a two-step method for the diagnosis of melanoma by reflectance confocal microscopy. J Am Acad Dermatol 2009;61:216-29. [PubMed]
© 2011 Dermatology Online Journal