Two cases with nickel-induced oral mucosal hyperplasia: A rare clinical form of allergic contact stomatitis?
Published Web Location
https://doi.org/10.5070/D39gt0826vMain Content
Two cases with nickel-induced oral mucosal hyperplasia: A rare clinical form of allergic contact stomatitis?
Esen Özkaya MD, Goncagül Babuna MD
Dermatology Online Journal 17 (3): 12
Department of Dermatology and Venereology, Istanbul Medical Faculty, Istanbul University, Istanbul, Turkey. profeo@istanbul.edu.trAbstract
Allergic contact stomatitis (ACS) can occur with variable clinical presentations such as erythematous, erosive, and lichenoid forms. Burning mouth symptoms may also be a result of allergic contact stomatitis. Additionally, gingival hyperplasia has been reported in exceptional cases of ACS caused by dental metals. Here, two rare cases are presented of nickel-induced oral mucosal hyperplasia with gingival and upper palatal involvement from metal-porcelain crowns and metal-acrylic upper denture, respectively. In both cases the diagnosis was made on the basis of the positive patch test results to nickel sulfate and the regression of the lesions after removing the nickel containing dental materials. Nickel-induced ACS should be borne in mind in every case of oral mucosal hyperplasia appearing after dental procedures, especially in the presence of previous allergies and sensitization risks such as ear piercing. It might be further suggested to include this variant within the clinical forms of ACS.
Introduction
Allergic contact stomatitis (ACS) can occur in variable clinical presentations such as erythematous, erosive, and lichenoid forms [1]. Burning mouth may also be a manifestation of allergic contact stomatitis. Additionally, gingival hyperplasia has been reported in exceptional cases of ACS caused by dental metals [2, 3, 4]. Here we report two rare cases of nickel-induced oral mucosal hyperplasia and suggest that the hyperplastic form might also be included within the clinical forms of ACS.
Case reports
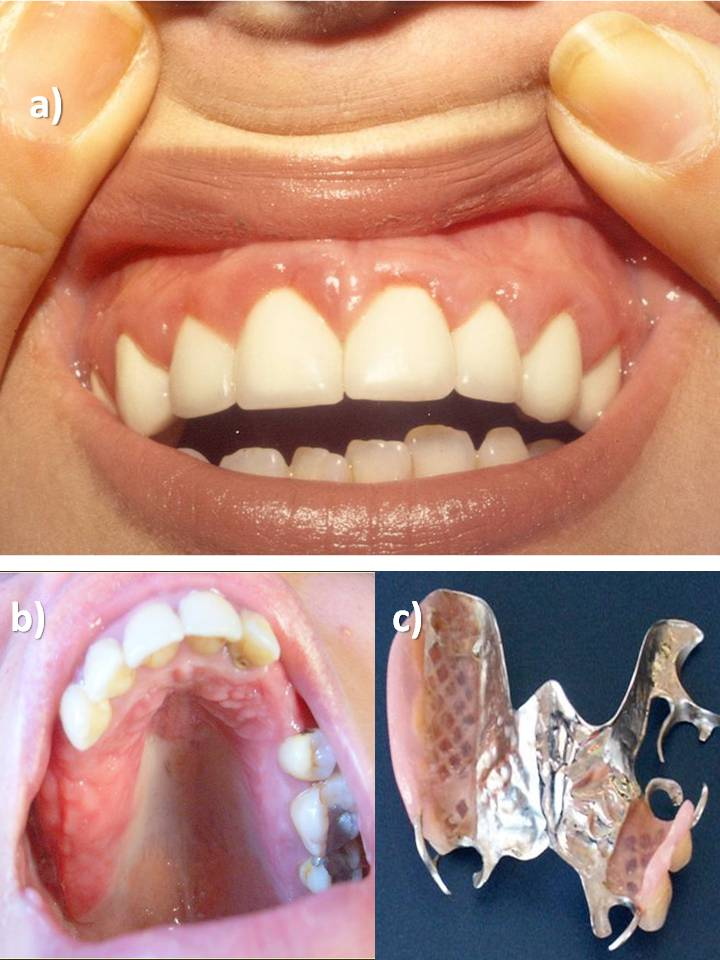
A 32-year-old non-atopic woman (Patient 1) was referred from a dentist because of recurrent gingival hyperplasia following the applications of nickel-chrome alloy-porcelain crowns. The first application had resulted in gingival overgrowth within 1 month. The crowns had been removed and the hyperplastic tissue had regressed within 3 weeks but it had redeveloped within four weeks following the application of new dental crowns having the same components as the former ones. Gingivectomies had been performed twice without removing the crowns and resulted in recurrence of gingival hyperplasia within a few weeks. Oral dermatologic examination revealed gingival hyperplasia surrounding the maxillary anterior crowns (Figure 1a).
 |
| Figure 1 |
|---|
| Figure 1. Gingival hyperplasia surrounding the maxillary incisors and canines following application of dental crowns containing nickel in Patient 1(a), mucosal hyperplasia on the hard palate (b) following application of a cobalt-chrome partial acrylic upper denture containing nickel in Patient 2 (c). |
Patient 2, a 36-year-old non-atopic woman, presented with reddened mucosal hyperplasia on the hard palate associated with burning sensation, pruritus, and bleeding, within 2 weeks following placement of a cobalt-chrome partial acrylic upper denture containing nickel, chrome, cobalt, and methyl methacrylate (Figures 1b and 1c). The Gram stain of a smear taken from the affected mucosa was negative for Candida albicans.
Both patients denied a lesional biopsy for histopathologic examination.
Using the International Contact Dermatitis Research Group criteria, patch testing showed a ++ positive reaction to nickel sulphate (5.0% pet.) at D2, D3, and D4 in both patients. It was negative for other ingredients of our extended European baseline series and dental series including the other components of dental appliances (Brial Allergen, Greven, Germany and Chemotechnique Diagnostics, Vellinge, Sweden).
Both patients had been exposed to nickel first in early childhood via ear piercing and gave a history of intolerance to jewelery. They were otherwise healthy. No drugs were used that could have caused oral mucosal hyperplasia such as cyclosporine, phenytoin, or calcium channel blockers.
Avoidance of nickel containing dental material resulted in complete regression of mucosal changes within 3 weeks in the first and 2 months in the second patient. The first patient could not be further contacted, whereas the second patient was free of lesions during a follow-up period of 8 months.
Discussion
The diagnosis of nickel-induced ACS in the form of oral mucosal hyperplasia was made in both cases on the basis of the positive patch test results to nickel sulphate and the regression of the lesions after removing the nickel containing dental materials.
Dental metals such as nickel, palladium, gold, and mercury mainly induce erythematous, erosive and lichenoid ACS [5, 6, 7, 8]. Although extremely rare, a hyperplastic form had also been reported in single cases from nickel in dental appliances [2, 3] and from gold and palladium in a dental clasp [4]. It might be difficult to differentiate an allergic mucosal hyperplasia from the trauma-induced or plaque-induced inflammation, the latter mainly related to poor oral hygiene. In experimental studies nickel was found to increase epithelial cell proliferation via induction of the synthesis of inflammatory cytokines and upmodulation of keratinocyte growth factor expression in keratinocytes [9]. It was further speculated that the sustained inflammation by metal allergy could induce proliferative cytokines for epithelia and connective tissue components, resulting in gingival hyperplasia [4].
Conclusion
In conclusion, nickel-induced ACS should be borne in mind in every case of oral mucosal hyperplasia appearing after dental procedures, especially in the presence of previous allergies and sensitization risks such as ear piercing. Cessation of the nickel exposure by removing the suspected dental appliance is then the only way of treatment. It might be suggested to include the hyperplastic variant within the clinical forms of ACS.
References
1. Tosti A, Pazzaglia M, Piraccini BM. Contact stomatitis. Available at: eMedicine (last accessed 16 September 2010).2. Kalkwarf KL. Allergic gingival reaction to esthetic crowns. Quintessence Int Dent Dig. 1984 Jul;15(7):741-5. [PubMed]
3. Counts AL, Miller MA, Khakhria ML, Strange S. Nickel allergy associated with a transpalatal arch appliance. J Orofac Orthop. 2002 Nov;63(6):509-15. [PubMed]
4. Kabashima K, Miyachi Y. Gingival hyperplasia due to metal allergy. Clin Exp Dermatol. 2005 Jan;30(1):88-9. [PubMed]
5. Khamaysi Z, Bergman R, Weltfriend S. Positive patch test reactions to allergens of the dental series and the relation to the clinical presentations. Contact Dermatitis. 2006 Oct;55(4):216-8. [PubMed]
6. Koch P, Bahmer FA. Oral lesions and symptoms related to metals used in dental restorations: a clinical, allergological, and histologic study. J Am Acad Dermatol. 1999 Sep;41(3 Pt 1):422-30. [PubMed]
7. Raap U, Stiesch M, Reh H, Kapp A, Werfel T. Investigation of contact allergy to dental metals in 206 patients. Contact Dermatitis. 2009 Jun;60(6):339-43. [PubMed]
8. Torgerson RR, Davis MD, Bruce AJ, Farmer SA, Rogers RS 3rd. Contact allergy in oral disease. J Am Acad Dermatol. 2007 Aug;57(2):315-21. [PubMed]
9. Gursoy UK, Sokucu O, Uitto VJ, Aydin A, Demirer S, Toker H, Erdem O, Sayal A. The role of nickel accumulation and epithelial cell proliferation in orthodontic treatment-induced gingival overgrowth. Eur J Orthod. 2007 Dec;29(6):555-8. [PubMed]
© 2011 Dermatology Online Journal