Hyperkeratotic Bowen disease - a case report
Published Web Location
https://doi.org/10.5070/D38h88k004Main Content
Hyperkeratotic Bowen disease - a case report
Shyam B Verma MD
Dermatology Online Journal 14 (6): 24
Amee Society, Gujarat, India. vermaderma@rediffmail.comAbstract
A 70-year-old woman of Indian descent, with Fitzpatrick type IV skin type, presented with a 1-year history of a hyperkeratotic facial plaque. She also exhibited numerous signs of chronic sun damage. Hyperkeratotic squamous cell carcinoma in-situ was diagnosed after skin biopsy. It is important to remember that darkly pigmented patients do develop skin cancers.
Case report
A 70-year-old woman of Indian descent presented in this clinic for a consultation regarding a "wart" that had been growing on her right temple for the past year. She also noticed a reddish scaly and rough lesion on the other side of the face between the left eye and the bridge of the nose. She had been a farm worker for 50 years and had significant long-term sun exposure. She had no complaints of any other skin problems.
 |  |
| Figure 1 | Figure 2 |
|---|
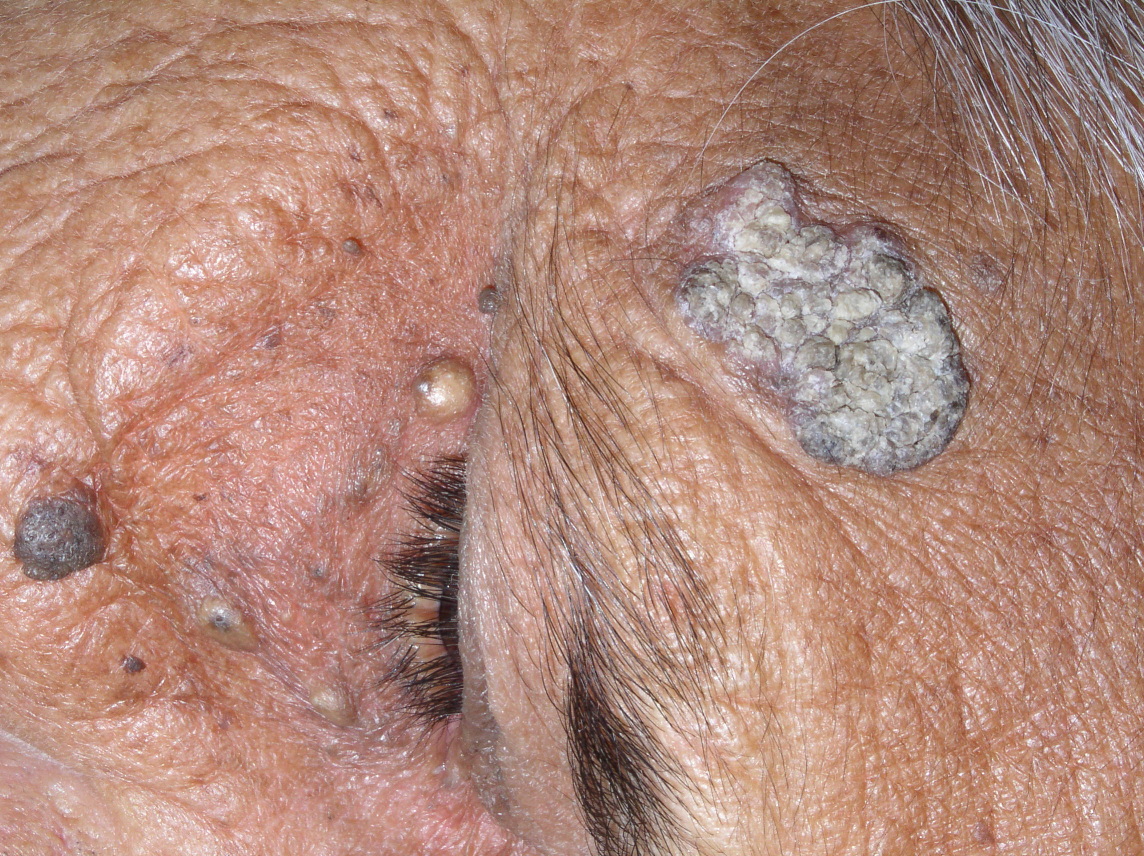
On examination the woman's face showed all the telltale signs of chronic actinic damage owing to her decades of work in the field. Her skin type was Fitzpatrick IV. Her skin had a sallow, waxy, weather-beaten appearance with accentuated creases, multiple seborrheic keratoses, and multiple comedones and cysts on her face, characteristic of Favre Racouchot syndrome. The primary lesion for which she sought consultation was on the right side of her temple. The plaque was about 3x2 cm in size, was well defined, rough, warty, pigmented and hyperkeratotic. There was no itching, no oozing, no bleeding, and no tenderness nor pain. The lesion was freely movable and there was no ulceration.
She also had a well defined erythematous macule on the left side of the face between the medial canthus of the eye and bridge of the nose of about 1x1 mm. The erythematous macule was topped by a scale that was thick and adherent in some areas of the lesion and free in other areas.
Clinically a possibility of superficial basal cell carcinoma (Pagetoid variant), hypertrophic Bowen disease, or verrucous carcinoma was entertained. The lesion was biopsied. The histopathology was characteristic of hyperkeratotic Bowen disease with full thickness dysplasia, a perfectly intact dermoepidermal junction, and no invasion. The lesion on the other side was an actinic keratosis that was was excised by the biopsy. The hyperkeratotic Bowen disease plaque was excised with a 4 mm margin and the patient did not show any recurrence at 1-year follow up. She has been advised to return every 6 months for follow up, reduce sunlight exposure, and apply sunscreens.
Discussion
Multiple stigmata of significant chronic solar exposure can occur in individuals with Fitzpatrick type IV skin. Three sun-related entities, hypertrophic Bowen disease, hyperkeratotic actinic keratosis, and Favre Rachouchot occurred in the same individual.
Although seborrheic keratoses and solar comedones are relatively common in darkly pigmented individuals, actinic keratoses and Bowen disease are not. Bowen disease is an intraepithelial carcinoma and chronic sunlight exposure is considered the most important cause in its development when located in sun-exposed areas [1, 2]. When it is seen on palms and soles or covered areas it is important to rule out exposure to arsenic [2]. It can occur on any area of the skin or the mucosa and presents as a chronic, erythematous, scaly, well-circumscribed plaque, usually without symptoms. Bowen disease may show many morphological and histological subtypes. Psoriasiform, atrophic, verrucous, hypkeratotic and irregular variants have been reported [1, 3, 4, 5]. Hyperkeratotic, verrucous and pigmented variants have often been reported on areas other than the face [6, 7, 8]. Pigmented and verrucous lesions have been reported over genitalia and in subungual locations, mimicking melanoma. The histology of hyperkeratotic Bowen disease is confirmatory showing profound hyperkeratosis and a full thickness atypia with an intact dermoepidermal junction [3]. Treatment includes destructive modalities such as curettage and electrodessication or cryotherapy, which are usually effective. Local cytotoxic agents such as 5-fluorouracil are efficacious, too. Photodynamic therapy using topical aminolevulinic acid and laser or non-laser light sources may also be effective [1]. We performed an excisional surgery with a cosmetic closure leaving a safe margin. This is an accepted and effective modality and is practical in a resource-poor country with its inherent problems of poor patient compliance and lack of regular follow-up.
This case points out the fact that darkly pigmented people, need to be screened regularly for solar damage and cutaneous malignancies. Farm workers living in villages often have no access to dermatologists unless they come to urban areas; they do not seek dermatologic treatment routinely. We and our colleagues in allied branches need to remind ourselves that although the incidence of cutaneous malignancies is decidedly lower in dark-skinned people compared to the skin types I, II and III, sun-related skin cancers may still develop. Such a possibility is always to be entertained and a biopsy should be taken of any suspicious lesion. Also, the longevity of males and females in India is increasing. This means we continue to have an increasing elderly population that needs to be screened for skin cancers. Transplant surgeries are now becoming more and more popular in India and that suggests the possibility of an increasing number of skin cancers. It appears worthwhile for all of us involved in skin care to be vigilant about the possibility of premalignant lesions and various cutaneous malignancies in highly pigmented individuals. This is especially true because we do not expect them and may overlook these because the patient has come in with unrelated complaints. A thorough skin screening, especially in older individuals, is necessary even in countries where people with predominantly skin types IV and V reside.
Acknowledgement: I thank Dr. Mayur Jani, plastic surgeon, Vadodara, for his surgical intervention.
References
1. MackKie RM and Quinn AG, in Non-Melanma Skin Cancer and Other Epidermal Skin Tumors In Textbook of Dermatology. 7th edn., Burns T, Breathnach S, Cox N et al. Vol II, Blackwell Publishing. Oxford..2004. 36.33-62. Andrews' 655-656 andrews' disease of the skin clinical dermatology. James W, Berger T, Elston D, Xth ed. Saunders Elsevier 2006: 655-656
3. McKee P, Calonje E, Granter S, Pathology of the skin. Vol II. 2005. Elsevier. Tumors of the surface epithelium. 1193-97
4. Hernández-Pérez, Enrique & Figueroa, Dagoberto Espinoza (2005). Warty and clear cell Bowen disease. International Journal of Dermatology 44 (7), 586-587 PubMed [PubMed - indexed for MEDLINE]
5. Dawn G, Das A, Kumar B: Uncommon presentations of Bowen disease.Ind J of Dermatol 1995 Jan-Mar.; 40(1): 42-4
6. Papageorgiou PP, Koumarianou AA, Chu AC. Pigmented Bowen disease; Br J Dermatol. 1998 Mar;138(3):515-8. PubMed [PubMed - indexed for MEDLINE]
7. Schamroth JM, Weiss RM, Grieve TP .Verrucous Bowen disease in a black patient. A case report. S Afr Med J. 1987 18;71(8):527-8. PubMed [PubMed - indexed for MEDLINE]
8. Grekin RC, Swanson NA. Verrucous Bowen disease of the plantar foot. J Dermatol Surg Oncol. 1984 Sep;10(9):734-6 PubMed [PubMed - indexed for MEDLINE]
© 2008 Dermatology Online Journal