Intra-anal condyloma: Surgical or topical treatment?
Published Web Location
https://doi.org/10.5070/D38df2772rMain Content
Intra-anal condyloma: Surgical or topical treatment?
Caterina Dianzani1, Alessandra Pierangeli4, Alessandra Avola1, Domenico Borzomati3, Paolo Persichetti2, Anna Marta Degener4
Dermatology Online Journal 14 (12): 8
1. Department of Dermatology, "Campus Biomedico," University of Rome, Italy. c.dianzani@unicampus.it2. Plastic Surgery, "Campus Biomedico," University of Rome, Italy
3. General Surgery "Campus Biomedico," University of Rome, Italy
4. Department of Experimental Medicine, Section of Virology, "Sapienza" University, Rome, Italy
Abstract
Human Papillomavirus infections are the strongest risk factors for genital cancer and are the causative agents of anogenital warts. Although the viral types associated with condylomata usually do not cause carcinoma, in women with a history of these lesions there is an increased risk of intraepithelial neoplasia and cancer. Generally the lesions are not life-threatening, but they provoke significant morbidity, are difficult to treat, and are a source of psychosocial stress. Thus, condylomata represent not only a health problem for the patient but also an economic burden for the society. Considering the individual episodes of care, men experience a longer duration of the lesions and incur greater costs than women. We report a case of a male patient with external and intra-anal condyloma resistant to laser therapy. Initially, surgical intervention appeared required because of florid and intra-anal growth. HPV DNA testing and sequencing revealed the presence of HPV 6. After initial discomfort, the lesions were successfully cleared with topical imiquimod 5 percent cream therapy.
Introduction
Human Papillomavirus (HPV) infection is one of the most common sexually transmitted diseases worldwide, with a prevalence of less than 10 percent to about 70 percent among heterosexual men with a similar incidence in women. Although most of the viral types associated with genital warts do not cause cancer, in women with history of condylomata, there is an increased risk of intraepithelial neoplasia and carcinoma associated with certain types.
Anogenital condylomata associated with low risk HPV types (HPV 6 or 11), can cause clinical symptoms such as burning, itching, bleeding, and pain. Moreover, the diagnosis of condylomata may cause psychological anxiety and embarrassment. Anogenital warts represent about 90 percent of genital HPV-associated diseases with high morbidity and substantial healthcare costs. In fact, the lesions frequently present high recurrence rates even after different ablative (electrocautery, liquid nitrogen, and laser therapy) treatments or surgical excision; men experience a longer duration of the lesions.
Case Report
In May 2006, a 41-year-old Caucasian, heterosexual, HIV-negative man was referred to the Department of Plastic Surgery and Dermatology of the University "Campus Bio-Medico" of Rome for numerous large, vegetative, anal ulcerated lesions of the perianal skin region (extending 15 cm in diameter). The warts extended into the anus up to the dentate line. Symptoms were extremely unpleasant for the patient who reported pain and itching of the anogenital warts and the discharge of purulent, bloody secretions constantly. A biopsy of the lesion was taken and histological analysis revealed hyperkeratosis and inflammatory infiltrate. After three weeks of anti-inflammatory treatment the patient was clinically evaluated by the dermatologist and a second biopsy was performed supporting the clinical suspicion of anal condyloma. Lymphocyte count revealed no alteration (WBC 10.5; Neutrophils 54%, Lymphocytes 34.7%) and there was no evidence of alteration in lymphocytes subgroups.
Promptly the condylomata were treated with CO2 laser (one treatment per week for six consecutive weeks). From the time of the initial diagnosis and in spite of several attempts at CO2 laser ablative treatment, several recurrences were recorded. Recurrences were probably caused by the incomplete ablation of the entire condyloma inside the anal canal up to the dentate line.
In October 2006 the blood exams were repeated and showed:
- Sum of cell (T+B+NK): 2.00 (Reference Range 0.9-3.6)
- Average T CD3+: 80 (Reference Range 59.4-84.6)
- Average T CD8+: 40 (R.R. 59.4-84.6)
- T helper CD3/CD4 ratio: 54 (R.R. 28.5- 60.5)
Moreover another biopsy was collected for Human Papillomaviruses (HPV) DNA testing. The Polymerase chain reaction (PCR) was performed with two sets of degenerated general primers as already reported [1]: the test gave a positive result. The sequence analysis revealed only the presence of HPV type 6.
The patient underwent colonoscopy that revealed an anal stretch with regular aspect, but distal papillomatosis to the dentate line. Abdominal and pelvic Nuclear Magnetic Resonance images were normal. At this time the extension and the persistence of the disease (Fig. 1A) lead to consideration of surgical treatment consisting of abdomen-perineal resection with graft reconstruction and permanent colostomy [2, 3].
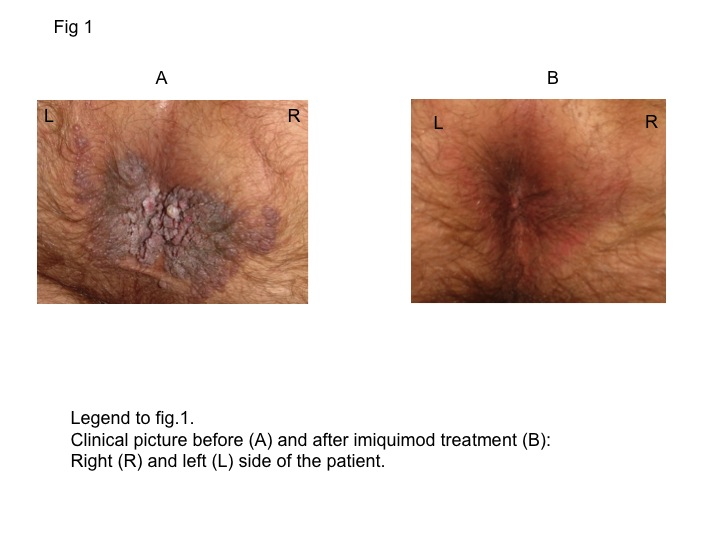 |
| Figure 1 |
|---|
However, considering the relatively young age of the patient and his persistent but non-malignant disease, a less invasive treatment with local imiquimod cream was attempted. Imiquimod is an immune response modulator approved by the U.S. Food and Drug Administration as a 5 percent cream; initially it was formulated as an antiviral agent, but its effects on the immune system (activation of antigen presenting cells induced by cytokine production and promotion of tumor antigen presentation) has permitted new treatment options [4, 5]. Imiquimod cream has also been successfully used in the treatment of premalignant (actinic keratosis) and malignant lesions such as perianal Bowen disease and erythroplasia of Queyrat on the glans penis [6, 7].
In this case, the topical formulation, five percent cream, was applied locally and partially inside the anal canal three times a week for a period of 16 weeks. Significant side effects in the initial period of treatment were constant pain, bleeding, burning sensation, itching, and pre-evacuative discomfort. Topical antibiotic unguent, zinc oxide cream, and diet modifications (to induce softening of feces) reduced the symptoms that gradually disappeared. Having completed the treatment, the patient returned for follow-up visits every month for six months and every two months in the following year. During this period, no symptoms were reported and there were no signs of recurrence. (Fig. 1B). At the last clinical examination in April, 2008 no recurrence was revealed; colonoscopy and NMR were negative.
Discussion
In the literature there are reports of severe cases of condylomata primarily treated with ablation or surgical methods and then with imiquimod to prevent recurrences. In other cases, anogenital warts were pre-treated with imiquimod and then treated by surgical excision to eliminate the residual warts [8, 9]. External condylomata can be effectively treated with local therapy, but infiltrative and recurrent lesions often require ablative and surgical treatments [10]. In young people, the trauma subsequent to surgical therapy may cause severe psychosocial stress.
We present a case of complete resolution of recurrent florid condylomata inside and outside the anal canal by topical imiquimod cream monotherapy. The reason for the unsuccessful laser treatments was probably due to the incomplete removal of the condyloma within the anal canal.
This case supports the importance of interdisciplinary collaboration. In fact the presence of a low-risk HPV and the characteristics of the patient (young age, immune-system status, absence of malignancy) encouraged us to try a topical treatment instead of surgical resection. It is important to evaluate all possible options, but it is often most judicious to begin with the less invasive treatment if possible in order to reduce psychological consequences for the patient and public health costs.
Acknowledgments: This work was partially supported by grant from MIUR-Italy (Ministero dell'Istruzione, Università, Ricerca scientifica).
References
1. Verteramo R, Pierangeli A, Calzolari E, Patella A, Recine N, Mancini E, Marcone V, Masciangelo R, Bucci M, Antonelli G, Degener AM. Direct sequencing of HPV DNA detected in gynaecologic outpatients in Rome, Italy. Microbes Infect. 2006 Aug;8(9-10):2517-21. Epub 2006 Jul 24. [PubMed]2. De Toma G, Cavallaro G, Bitonti A, Polistena A, Onesti MG, Scuderi N. Surgical management of perianal giant condyloma acuminatum (Buschke-Löwenstein tumor). Report of three cases. Eur Surg Res. 2006;38(4):418-22. [PubMed]
3. Trombetta LJ, Place RJ. Giant condyloma acuminatum of the anorectum: trends in epidemiology and management: report of a case and review of the literature. Dis Colon Rectum. 2001 Dec;44(12):1878-86. Review. [PubMed]
4. Gaspari AA. Mechanism of action and other potential roles of an immune response modifier. Cutis. 2007 Apr;79(4 Suppl):36-45. Review. [PubMed]
5. Sauder DN. Immunomodulatory and pharmacologic properties of imiquimod. J Am Acad Dermatol. 2000 Jul;43(1 Pt 2):S6-11. Review. [PubMed]
6. Arlette JP. Treatment of Bowen's disease and erythroplasia of Queyrat. Br J Dermatol. 2003 Nov;149 Suppl 66:43-9. [PubMed]
7. Micali G, Nasca MR, De Pasquale R. Erythroplasia of Queyrat treated with imiquimod 5% cream. J Am Acad Dermatol. 2006 Nov;55(5):901-3. Epub 2006 Sep 14. [PubMed]
8. Kaspari M, Gutzmer R, Kaspari T, Kapp A, Brodersen JP. Application of imiquimod by suppositories (anal tampons) efficiently prevents recurrences after ablation of anal canal condyloma. Br J Dermatol. 2002 Oct;147(4):757-9. [PubMed]
9. Carrasco D, vander Straten M, Tyring SK. Treatment of anogenital warts with imiquimod 5% cream followed by surgical excision of residual lesions. J Am Acad Dermatol. 2002 Oct;47(4 Suppl):S212-6. Review. [PubMed]
10. Schöfer H. Evaluation of imiquimod for the therapy of external genital and anal warts in comparison with destructive therapies. Br J Dermatol. 2007 Dec;157 Suppl 2:52-5. Review. [PubMed]
© 2008 Dermatology Online Journal