Cerebriform intradermal nevus presenting as secondary cutis verticis gyrata
Published Web Location
https://doi.org/10.5070/D38014p6pnMain Content
Letter: Cerebriform intradermal nevus presenting as secondary cutis verticis gyrata
Javier Alcántara González MD1, María Teresa Truchuelo Díez MD1, Rosario Carrillo Gijón PhD2, Rosa María Martín Diaz MD3, Pedro Jaén Olasolo PhD1
Dermatology Online Journal 16 (12): 14
1. Dermatology Department, Ramon y Cajal Hospital, Madrid, Spain2. Pathology Department, Ramon y Cajal Hospital, Madrid, Spain
3. Internal medicine, Fuenlabrada Hospital, Madrid, Spain
Abstract
Cutis verticis gyrata is a rare skin condition characterized by ridges and furrows resembling the surface of the brain. It can be considered as a manifestation of a variety of diverse causes such as cerebriform intradermal nevus. We report a 48-year-old man with cerebriform and soft folds on the left parietal and temporal areas. Histology showed solitary or clusters of nevus cells in the dermis. The diagnosis of cerebriform intradermal nevus was confirmed.
Introduction
Cutis verticis gyrata (CVG) is a rare skin condition characterized by ridges and furrows resembling the surface of the brain. It is usually located on the scalp, but other locations have also been reported, such as the neck, legs, buttocks, scrotum, or back [1, 2]. Cutis verticis gyrata can be considered a manifestation of a variety of causes rather than an individual disease. Accordingly, CVG is classified into primary and secondary. Primary CVG may be divided into essential CVG, if no other abnormalities are identified, and non-essential CVG, which can be associated with mental deficiency, cerebral palsy, epilepsy, seizures, or ophthalmological disorders [3].
The secondary form of CVG is caused by an underlying condition, such as amyloidosis, syphilis, acromegaly [4], myxedema, pachydermoperiostosis [5], neurofibroma, giant congenital melanocytic nevus (GCMN) [2], or cerebriform intradermal nevus (CIN) [6, 7, 8, 9].
Case report
 |
| Figure 1 |
|---|
| Figure 1. Ridges and furrows with mild alopecia on the left hemicranial region |
We present a 48-year-old healthy man who was referred because of redundant skin on the left hemicranial area (Figure 1). He first noticed this condition about 30 years prior to presentation after a haircut. The patient reported that the lesion grew until he was 25 years of age, but there have been no significant changes since then. No previous trauma was reported. His medical history was not significant and he denied family history of similar disorder.
Physical examination revealed several cerebriform and soft folds located on the left parietal and temporal areas of the scalp. Slight hyperpigmentation and alopecia could be observed over them. Laboratory results, including VDRL, serum level of growth hormone, and thyroid function, were all negative or normal. A skin biopsy specimen showed solitary or clusters of nevus cells containing varying amounts of melanin in the papillary and deep reticular dermis without a junctional component (Figure 2). Neuroid transformation was present at the bottom of the lesion (Figure 3).
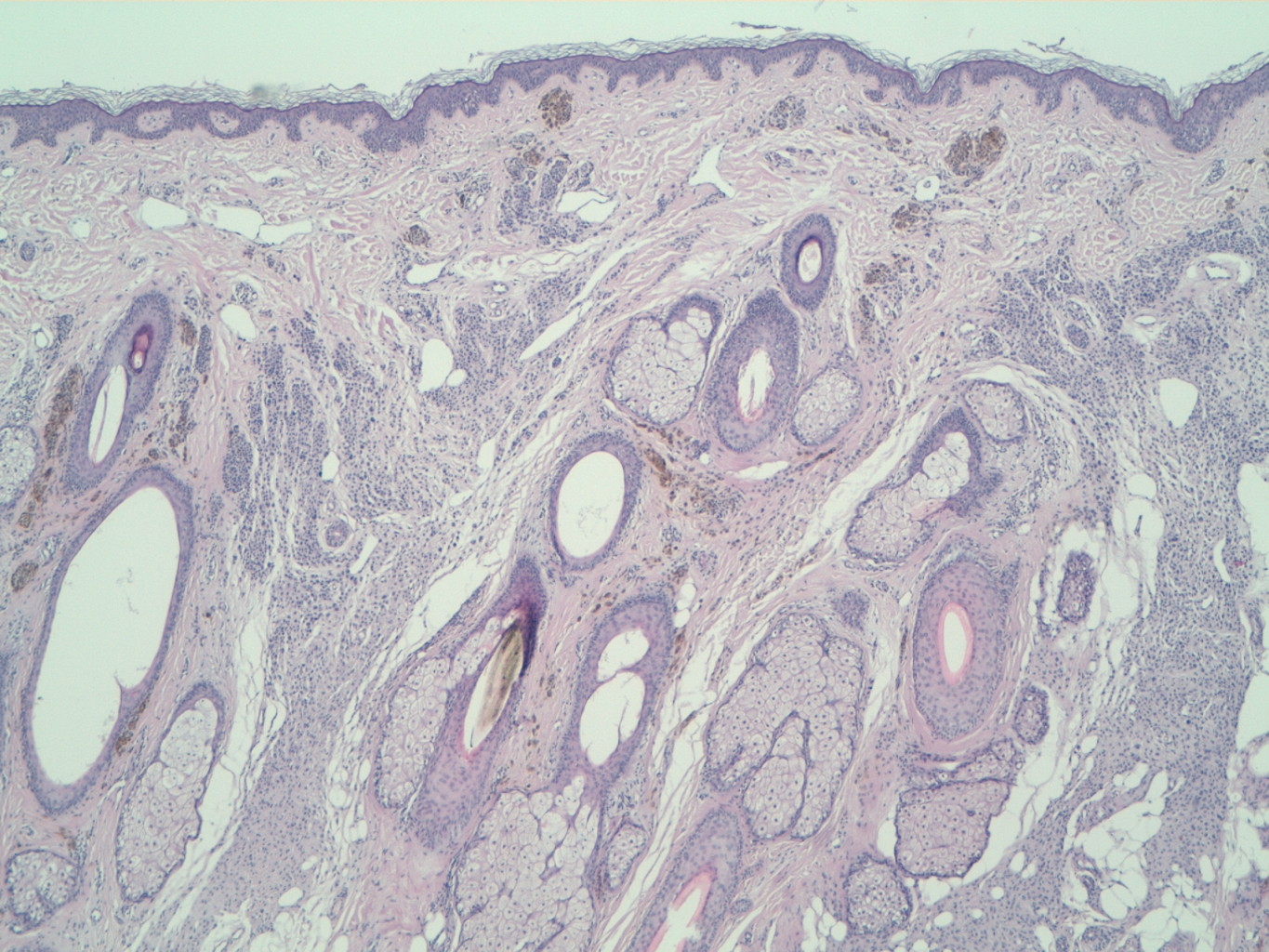 | 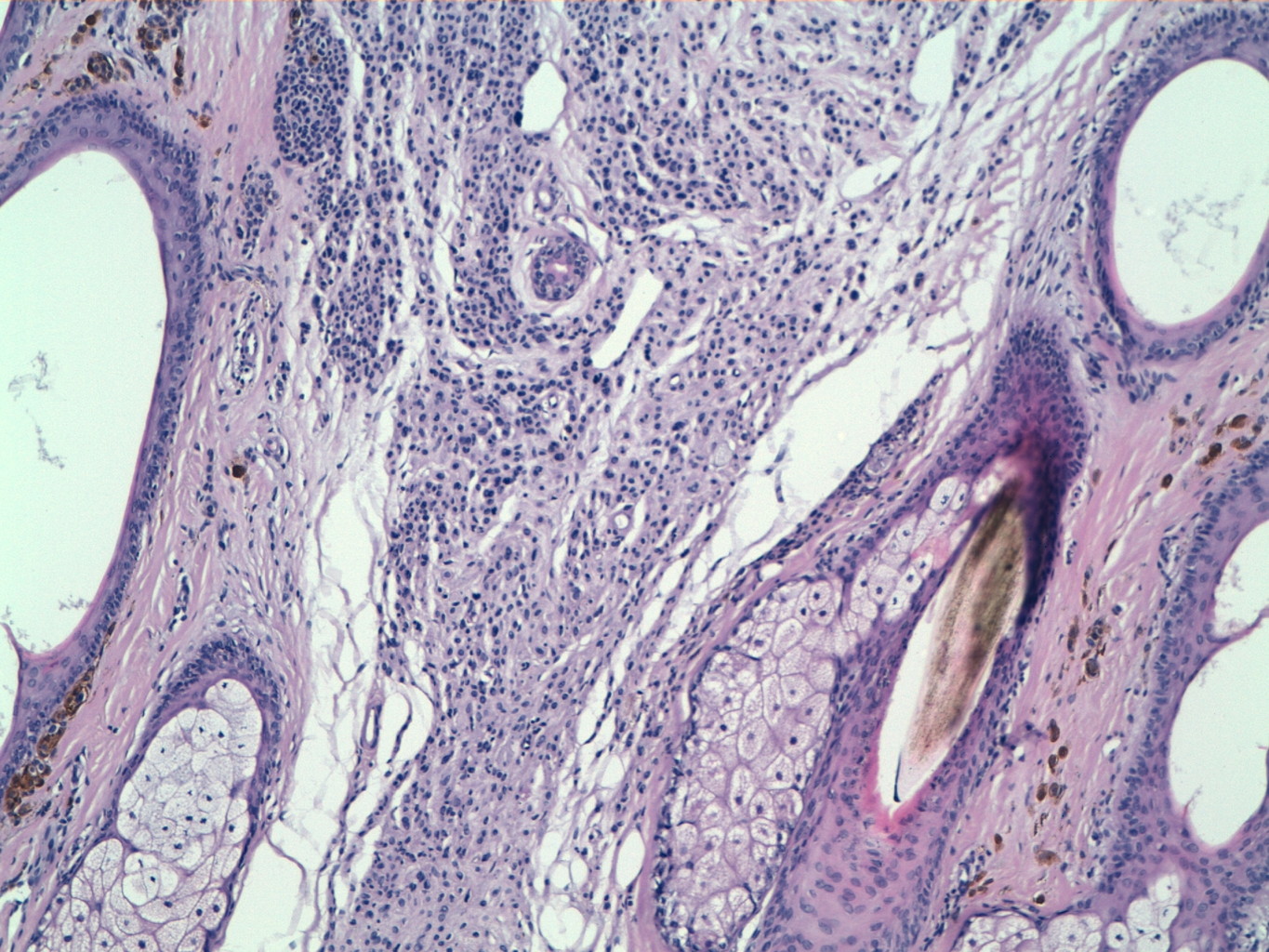 |
| Figure 2 | Figure 3 |
|---|---|
| Figure 2. Nevus cells nests with different degrees of pigmentation reaching deep portions of reticular dermis (H&E) Figure 3. Neuroid transformation of nevus cells in deeper interfollicular areas of the dermis (H&E) | |
The diagnosis of cerebriform intradermal nevus was made according to the clinical and histopathologic findings. Because of the large size of the nevus, surgical treatment was rejected.
Annual follow-up is being conducted for an early detection of possible malignant transformation to melanoma.
Discussion
Cerebriform intradermal nevus is a rare disorder that usually presents at birth or early life. It is a rare cause of secondary CVG or pseudo-CVG. Cerebriform intradermal nevus appears as an asymmetric, skin colored, or slightly pigmented tumor that is usually localized in the parietal or occipital areas of the scalp. Over the years, the nevus slowly enlarges and becomes more prominent. Pregnancy, surgical exploration, and hormonal activity have been related to the growth of these lesions. No systemic diseases have been associated with cerebriform intradermal nevus to date [8].
Histological examination shows intradermal nevus cells present in the full thickness of the dermis. The nests of nevus cells can be well delineated or irregular. Neuroid transformation can be present in the deeper parts of the lesion with increased collagen fibers. Hair follicles can be normal or atrophic.
Cerebriform intradermal nevus and giant congenital melanocytic nevus are thought to be related conditions by some authors. They share similar histopathologic features, but they have several differences. Giant congenital melanocytic nevus has intense pigmentation, an increased number of hair follicles and frequent nevus cell nests at the dermoepidermal junction, whereas cerebriform intradermal nevus is usually a slightly or non-pigmented lesion, with absent or sparse hair follicles, and uncommon junctional activity [7].
An uncommon progression to melanoma has been reported in giant cerebriform nevus [4, 8]. Surgical excision and plastic reconstruction are frequently performed because of the risk of malignant transformation and aesthetic reasons. When they are not possible, close follow-up is mandatory.
Neurocutaneous melanosis is a rare congenital syndrome characterized by the development of large or multiple congenital melanocytic nevi and benign or malignant melanocytic tumors of the central nervous system [10]. Neurologic manifestations within the first 2 years of life are seen in 58 percent of patients, but are uncommon after the second decade of life (8% of patients) [11]. The outcome of symptomatic neurocutaneous melanosis is very poor and there is no effective treatment. Cerebriform intradermal nevus has been related to giant congenital melanocytic nevus. However, the risk of neurocutaneous melanosis in patients with cerebriform intradermal nevus has not yet been established.
Because of the absence of neurological symptoms and the age of our patient, the lack of effective treatment, and the unknown relation between cerebriform intradermal nevus and neurocutaneous melanosis, we did not consider it necessary to perform a magnetic resonance imaging study.
References
1. Yazici AC, Ikizoglu G, Baz K, Polat A, Ustunsoy D. Cerebriform intradermal nevus. Pediatr Dermatol. 2007 Mar-Apr;24(2):141-3. [PubMed]2. Quaedvlieg PJ, Frank J, Vermeulen AH, Toonstra J, van Neer FJ. Giant ceribriform intradermal nevus on the back of a newborn. Pediatr Dermatol. 2008 Jan-Feb;25(1):43-6. [PubMed]
3. Larsen F, Birchall N. Cutis verticis gyrata: three cases with different aetiologies that demonstrate the classification system. Australas J Dermatol. 2007 May;48(2):91-4. [PubMed]
4. Al-Bedaia M, Al-Khenaizan AS. Acromegaly presenting as cutis verticis gyrata. Int J Dermatol. 2008 Feb;47(2):164. [PubMed]
5. Thappa DM, Sethuraman G, Kumar GR, Elangovan S. Primary pachydermoperiostosis: a case report. J Dermatol. 2000 Feb;27(2):106-9. [PubMed]
6. van Geest AJ, Berretty PJ, Klinkhamer PJ, Neumann HA. Cerebriform intradermal naevus (a rare form of secondary cutis verticis gyrata). J Eur Acad Dermatol Venereol. 2002 Sep;16(5):529-31. [PubMed]
7. Yazici AC, Ikizoglu G, Baz K, Polat A, Ustunsoy D. Cerebriform intradermal nevus. Pediatr Dermatol. 2007 Mar-Apr;24(2):141-3. [PubMed]
8. Hamm JC, Argenta LC. Giant cerebriform intradermal nevus. Ann Plast Surg. 1987 Jul;19(1):84-8. [PubMed]
9. Lasser AE. Cerebriform intradermal nevus. Pediatr Dermatol. 1983 Jul;1(1):42-4. [PubMed]
10. Kadonaga JN, Frieden IJ. Neurocutaneous melanosis: definition and review of the literature. J Am Acad Dermatol. 1991 May;24(5 Pt 1):747-55. [PubMed]
11. Covarrubias ER, López AG, Hernández AHM, Pineda FH. Melanosis neurocutánea. Presentación de un caso clínico, características clínicas y radiológicas. Bol Med Hosp Infant Mex. 2006 Mar-Abr;63:122-128.
© 2010 Dermatology Online Journal