Squamous cell carcinoma in chronic wound: Marjolin ulcer

Main Content
Squamous cell carcinoma in chronic wound: Marjolin ulcer
Vanessa Cocchetto MD, Paula Magrin MD, Roberta Andrade de Paula MD, Márcia Aidé MD, Leonardo Monte Razo MD, Luciana Pantaleão
MD
Dermatology Online Journal 19 (2): 7
Universidade Federal Fluminense, Rio de Janeiro, BrazilAbstract
Cutaneous squamous cell carcinoma (SCC) is a malignant tumor that can occur in normal skin, but commonly evolves from precursor lesions. SCC arising in ulcers is a rare and often aggressive cutaneous malignancy that arises from chronic wounds or old scars and is the most common histological tumor type found in Marjolin ulcer. Most frequently occurs in patients of low socioeconomic status, with limited access to health services, as a result of burns and other neglected injuries. Herein, we report a case of squamous cell carcinoma originating from a longstanding decubitus ulcer in a 56-year-old paraplegic man.
Introduction
Cutaneous squamous cell carcinoma (SCC) is a malignant tumor derived from Cutaneous squamous cell carcinoma (SCC) is a malignant tumor derived from suprabasal epidermal keratinocytes, with invasive nature and potential to metastasize [1, 3] and is the tumor type of 15 percent of malignant epithelial neoplasms [1]. It can occur in normal skin, but often develops from precancerous lesions, particularly actinic keratoses and Bowen disease, but also from actinic cheilitis, leukoplakia, radiation dermatitis, arsenical keratosis, xeroderma pigmentosum, chronic ulcers, burn scars, and erosive oral lichen [1, 3, 4]. Marjolin ulcer is a rare and often aggressive cutaneous malignancy that arises from chronic wounds or old scars, and the most common histological tumor type found is SCC [7]. The transformation from ulcer to malignant disease is typically slow and the pathogenesis is unknown [6]. Identification of risk factors and a high index of suspicion are the key to early diagnosis. Chronic wounds should be regularly monitored for evidence of malignant transformation. In the clinical exam, noting any change in appearance of the scar or ulcer necessitates histological assessment. As with most tumors, early treatment results in the best prognosis [7].
Case report
A 56-year-old man, born and raised in São Gonçalo, state of Rio de Janeiro, Brazil, paraplegic for 30 years because of spinal cord injury, reported the existence of a pressure ulcer in his sacral region for nearly 10 years. Three years prior to presentation he noticed the onset of a vegetating lesion arising from the ulcer, with progressive growth since then. His main complaints were local pain and foul smell. The patient reported no comorbidities, but he appeared to be underweight. Upon dermatological examination we observed an exuberant vegetating tumor with irregular edges, measuring approximately 15 x 12 cm, affecting the sacral region (Figures 1 and 2).
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figures 1 and 2. Exuberant vegetations on sacral region | |
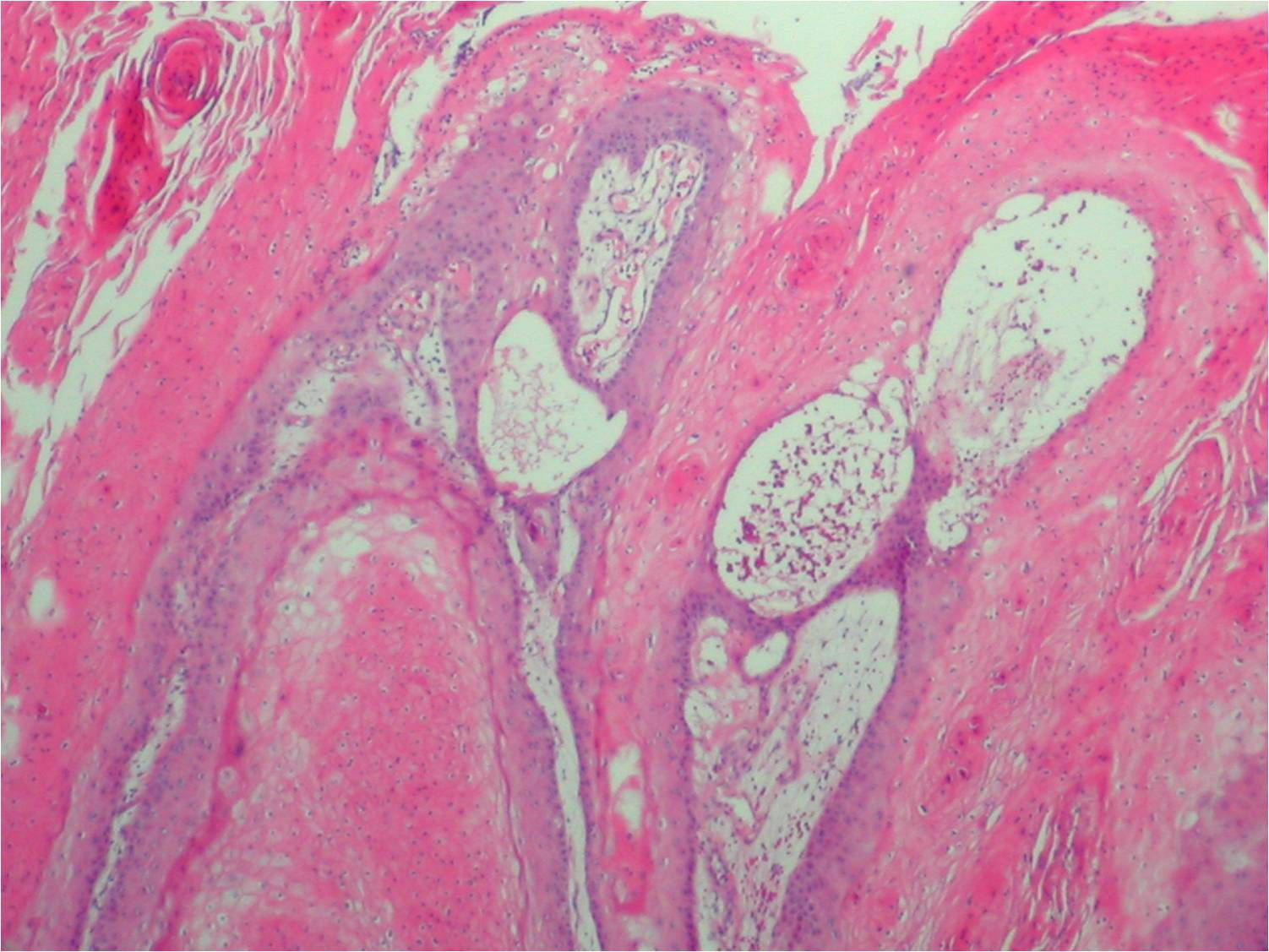
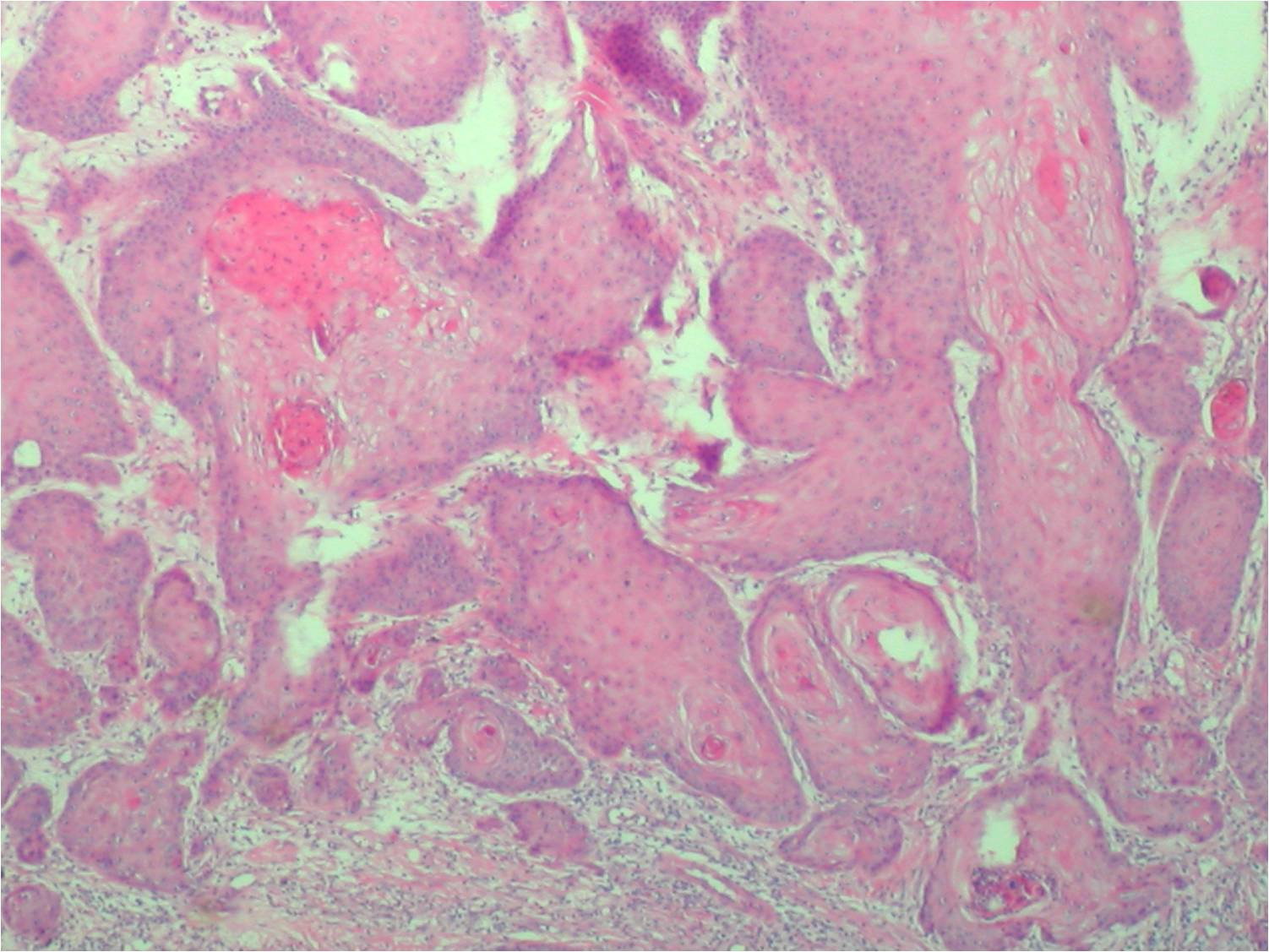
A biopsy was performed and a well-differentiated squamous cell carcinoma was confirmed (Figures 3 and 4). The infiltrative pattern areas were key to differentiate SCC from verrucous carcinoma. Although verrucous carcinoma is considered a form of well-differentiated SCC, the former has distinct histopathological characteristics [9, 10].
 |  |
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. Papillary architecture, with parakeratosis, dilated vessels in the dermal papillae and minimum cytologic atypia.
(x100) Figure 4. In the depth of the lesion there are infiltrative pattern areas, with the presence of “keratin pearls.” (x100) | |
Computed tomography (CT) revealed tumor infiltration into the deep dermis and subcutaneous tissue, apparently without bone involvement. Bilateral inguinal lymphadenopathy was present, but all lymph nodes were negative after fine needle aspiration biopsy. Surgery was scheduled but unfortunately the patient had severe pneumonia and died before it could happen.
Discussion
Marjolin's ulcer is a rare and often aggressive cutaneous malignancy that arises in previously traumatized, degenerated and chronically inflamed skin or scar tissue [7]. It is commonly associated with burn scars, but may develop from pressure sores, chronic venous ulcers, traumatic wounds, osteomyelitis, fistulas, and leprosy ulcers [6, 7, 8]. The most common histological tumor type is squamous cell carcinoma, but basal cell carcinomas, melanomas, and sarcomas may also be found [7]. Marjolin's ulcers occur at any age and in all races. Men are more affected than women with a ratio of about 3:1. The latent period between injury and the development of cancer is typically long, with an average of 31 years [7]. The pathogenesis of malignant transformation is still unknown and its risk factors include healing by secondary intention, wound infection, fragile and easily traumatized tissue, and poor local and systemic immune resistance [7]. Identification of risk factors and clinical suspicion are essential for early diagnosis. The tumor potential for development from several types of wounds and different anatomical sites, combined with the difficulty of diagnosis without biopsy, may delay proper treatment in many cases. Marjolin ulcers most frequently occur in patients of low socioeconomic status, with limited access to health services, and as a result of burns and other neglected injuries. Most of the cases reported are from developing countries, where patients tend to have late presentations [6]. Malignant change appears to be preventable if early wound coverage is undertaken [6]. Wide local excision and subsequent grafting seems to be the standard procedure for most authors. If closure is not possible, the wound must be closely evaluated for evidence of malignant transformation with biopsy at regular intervals. If squamous cell carcinoma is found, wide excision is indicated and attention to lymph node evaluation and examination for distant metastasis should be addressed [6]. Moreover, radiotherapy and chemotherapy can be used as adjuvant, or in extensive cases, palliative therapy. Recurrence rates are high despite current treatment advances and appropriate long-term follow-up is mandatory. Recurrences are almost always local but metastases to the lungs, brain, liver, and distant lymph nodes have been reported [7]. The prognosis of Marjolin's ulcer is related to the local extent of disease, location, histological types, and degree of differentiation, patient immune status, latency period, and, most importantly, the presence of lymph node metastases. The SCC originating from chronic ulcers is locally and systemically more aggressive than other types of SCC [7].
References
1. Sampaio, S.P.A., Rivitti,E.A., Dermatologia, 3ed., São Paulo:Editora Artes Médicas, 2007.2. Bologna,J., Jorizzo, J., Rapini, R.P., Dermatologia, 2ed., Rio de Janeiro:Editora Elsevier, 2010.
3. Klaus Wolff, Lowell A. Goldsmith, Stephen I. Katz, Barbara A. Gilchrest, Amy S. Paller, David J. Leffell. Fitzpatrick’s Dermatology in General Medicine. 7ed. McGraw-Hill Brasil, 2008.
4. Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook’s Textbook of Dermatology. Massachusetts:Blackwell; 2004.
5. Esther, R.J., Lamps, L., Schwartz, H.S. Marjolin ulcers: secondary carcinomas in chronic wounds. J South Orthop Assoc. 1999; 8(3): 181-7. [PubMed]
6. Kerr-Valentic, M.A., et al. Marjolin’s Ulcer: modern analysis of an ancient problem. Plast Reconstr Surg. 2009 Jan; 123(1): 184-191. [PubMed]
7. Daya M & Balakrishan T. Advanced Marjolin’s ulcer of the scalp in a 13-year-old boy treated by excision and free tissue transfer: Case report and review of literature. Indian J Plast Surg. 2009 Jan-Jun; 42(1): 106-111. [PubMed]
8. Copcu, E. Marjolin’s Ulcer: A Preventable Complication of Burns? Plast Reconstr Surg. 2009 Jul; 124(1):156e i 164e. [PubMed]
9. Weedon. Weedon’s Skin Pathology. Brisbane: Elsevier, 2010.
10. Mckee P, Calonje E, Scott G R. Pathology of the Skin with Clinical Correlations. Boston: Elsevier, 2011.
© 2013 Dermatology Online Journal