Erythema elevatum diutinum: An “idiopathic” case
Published Web Location
https://doi.org/10.5070/D37r2780p7Main Content
Erythema elevatum diutinum: An “idiopathic” case
Nadia El Fekih MD1, Ikram Belgith MD1, Bécima Fazaa MD1, Soumeya Remmah MD2, Faten Zéglaoui MD1, Rachida Zermani MD2, Mohamed Ridha Kamoun MD1
Dermatology Online Journal 17 (7): 7
1. Departement of Dermatology, Charles Nicolle Hospital, Tunis, Tunisia2. Departement of Anatomopathology, Charles Nicolle Hospital, Tunis, Tunisia
Abstract
Erythema elevatum diutinum (EED) is a rare condition with an unclear pathogenesis. Initially classified within neutrophilic dermatoses, it is now considered as a leukocytoclastic vasculitis accordingly to its histopathologic pattern. Several clinical presentations as well as many associated diseases are reported in the literature. We report a new case of EED in a 58-year-old man who presented with a three-month history of plaques and nodules on the extensor surfaces of hands, elbows, knees, ankles, forearms, and buttocks. Histology showed a leucocytoclastic vasculitis, suggestive of the diagnosis of EED. Screening for an associated pathology, namely a paraproteinemia or a solid cancer, was negative. Treatment with dapsone leads to amelioration within few weeks.
Introduction
Erythema elevatum diutinum (EED) was first described in 1894. Since then, almost 250 cases have been reported in the literature. Erythema elevatum diutinum is now considered to be part of the spectrum of leukocytoclastic vasculitis. Clinically, it is characterized by red, brownish or violaceous plaques and nodules that usually have a symmetrical distribution on the extensor, articular surfaces of the extremities. Most cases of EED were described in association with hematological, auto-immune, systemic, neoplastic, or infectious underlying diseases, leading to the hypothesis of an immune-complex pathogenesis of this condition. We report an “idiopathic” case.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Fed-brown plaques on dorsum of hands and fingers Figure 2. Red-brown plaques on the extensor surfaces of knees | |
 |
| Figure 3 |
|---|
| Figures 3. Lesions of the buttocks |
We report the case of a 58-year-old man who presented with a three-month history of pruritic red-brown, firm plaques and nodules, slightly tender to the touch, on dorsum of hands and fingers (Figure 1), the extensor surfaces of elbows, knees (Figure 2), and ankles, as well as forearms, buttocks, and the Achilles area (Figure 3). The eruption was not associated with any systemic symptoms except moderate arthralgias of interdigital joints. The patient had a medical history of type 2 diabetes mellitus and chronic obstructive pulmonary disease treated by inhaled β-mimetic, corticosteroid, and oral theophylline.
 |  |
| Figure 4 | Figure 5 |
|---|---|
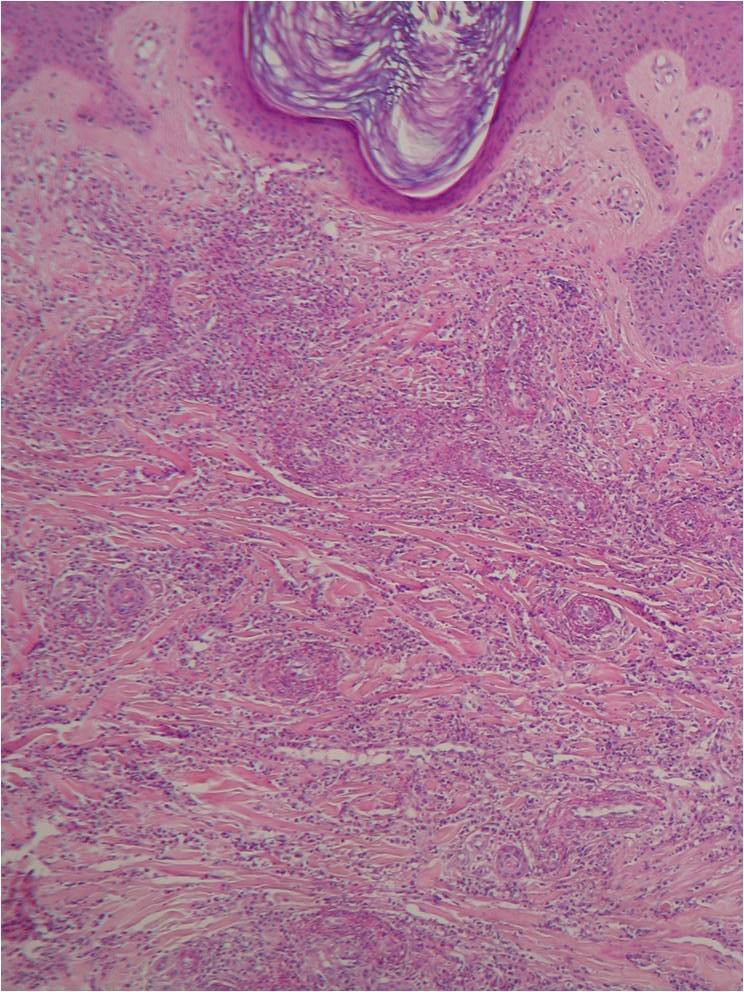
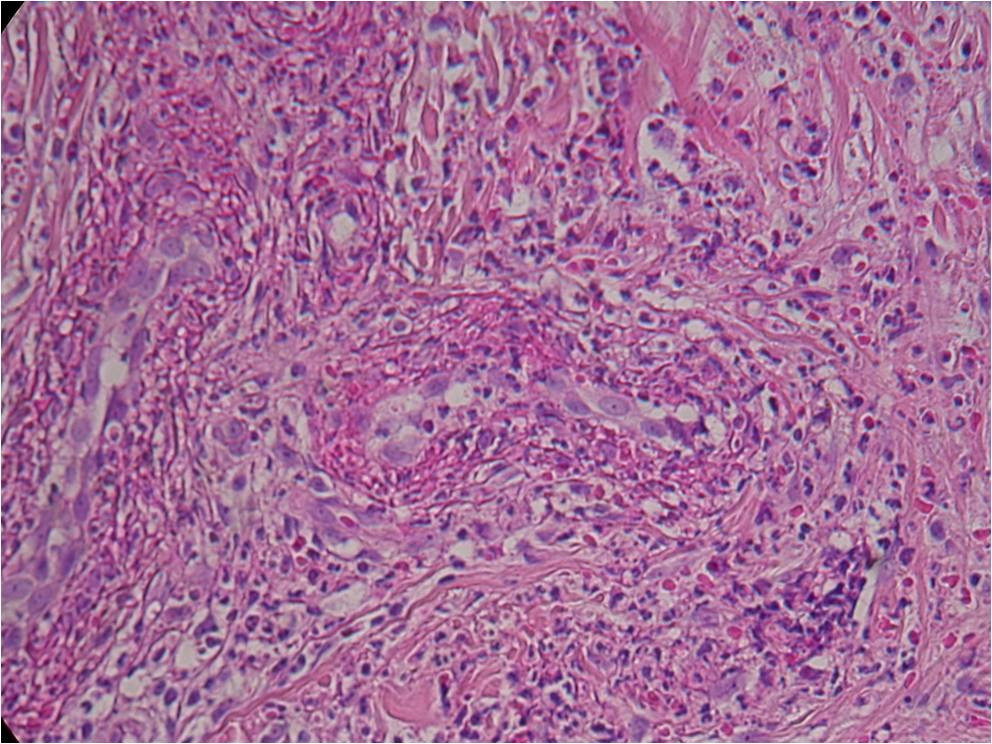
| Figure 4. Optical microscopy (x10): Leucocytoclastic vasculitis with a neutrophilic cell infiltrate in the dermal small vessels
walls Figure 5. Optical microscopy (x40): Leucocytoclastic vasculitis with a neutrophilic cell infiltrate in the dermal small vessels walls | |
A skin biopsy was performed in a plaque of the hand. It shows a leucocytoclastic vasculitis (LCV) with a neutrophilic cell infiltrate and fibrin deposits in the dermal small vessels walls (Figures 4 and 5).
Based on the clinical and histopathological findings, the diagnosis of EED was made.
Laboratory findings included a normal complete blood count, renal function tests, and liver function tests. Erythrocyte sedimentation rate was 27 mm/hr and C-reactive protein was normal. Anti-nuclear antibody was negative. Qualitative dosage of immunoglobulin and serum protein electrophoresis were both normal. HIV and viral hepatitis serologies were negative. Tumor markers: Prostate Specific Antigen (PSA), Carbohydrate Antigen (CA19-9), Alpha-fetoprotein (AFP), and Carcinoembryonic Antigen (CEA) were normal. A chest radiograph showed no abnormalities.
Treatment was started with dapsone 50 mg/day orally. After 4 weeks of treatment, we noticed a decrease in the thickness of plaques and nodules and a regression of pruritus and tenderness. The patient did not show any clinical or biological side effects.
Comments
Erythema elevatum diutinum is a rare chronic dermatosis. We have reported a case with typical clinical presentation and histological aspect.
Erythema elevatum diutinum can occur at any age but it appears that there is a peak in the sixth decade, with an equal sex ratio [1]. Clinically, the lesions present as firm, tender, brownish, red to purple papules, plaques, or nodules. The extensor aspects of the extremities, usually near joints such as the fingers, hands, elbows, ankles, and knees, are the preferred location for skin lesions. However, occurrences at atypical sites have been reported, including truncal, retroauricular, palmar, and plantar areas [2]. Uncommonly, the lesions may resemble vesicles, hemorrhagic nodules, ulcerations, or tumors [3, 4]. Erythema elevatum diutinum may also present as a solitary lesion [5]. The lesions of EED are usually asymptomatic, but pruritus, pain, and arthralgia of the involved joints have been reported.
The histological features observed in our patient, as leucocytoclastic vasculitis and neutophilic infiltrate, were characteristic. However, the lesions are not always as typical. Thus, correlation between the age of EED lesions and the histopathologic findings has been documented. Early lesions show vasculitis in which the predominant inflammatory cells are polymorphonuclear leukocytes with nuclear dust [6]. In older lesions, fibrosis predominates and may even form well-circumscribed nodules with a few foci of vasculitis [7]. Fibrotic lesions can include the deposition of lipid material, thought to consist in cholesterol esters. The degree of blood vessel destruction and leucocytoclasia do not predict the association with medical disorders [8].
Clinical and histopathologic similarities between EED and neutrophilic dermatosis, especially Sweet syndrome, are present. The lesions in both may begin as urticarial papules and progress to form tumid or firm plaques with bullae. Dermal neutrophilia is present in both, but EED is distinguished from other neutrophilic dermatoses by vasculitis.
Most cases of EED were reported in association with variable diseases, especially of an infectious, neoplastic or autoimmune origin. Streptococcal infection was the first disorder associated with EED after the isolation of streptococci from affected skin and reproduction of lesions after intradermal injection of streptococcal antigen. Since 1977, a marked association of EED with paraproteinemia, especially monoclonal IgA gammopathy and IgA myeloma has been reported [9]. In the review by Yiannias et al. about 13 patients with EED, 6 patients had a hematologic abnormality; IgA gammopathy was the most frequent (four patients) [8]. Erythema elevatum diutinum preceded the myeloproliferative disorders by an average of 7.8 years in this study. Even though blood screening was normal in our patient, long term monitoring is necessary to detect hematologic disorder early.
Not only IgA monoclonal gammopathy should be excluded in cases of EED. In fact, cases of EED were reported in association with IgM paraproteinemia, non-Hodgkin lymphoma [10], chronic lymphocytic leukemia [11], and hyperimmunoglobulinemia D syndrome [12].
Futei and Konohana reported one patient with EED and B-cell lymphoma, with complete healing of EED under chemotherapy for the lymphoma [13]. Hatzitolios also reported the complete regression of EED after the treatment of non-Hodgkin lymphoma with CHOP [10]. Two another cases of EED, one associated with pulmonary lymphoepithelioma-like carcinoma [14] and one with breast carcinoma [15], completely resolved after the treatment of the cancer. Those observations may lead to consider EED as a paraneoplastic syndrome.
More recently, many cases have been described in association with HIV infection, leading to suspect a non-fortuitous association. Antigen-antibody complexes from HIV might explain the pathogenesis of EED in those patients. On the other hand, the immunosuppression caused by HIV infection promotes other disorders, which are classically related to EED such as streptococcal infection or dysglobulinemia [5, 16, 17]. Kaposi sarcoma and bacillary angiomatosis are the principal diseases in the differential diagnosis of EED in HIV-infected patients. A case of EED associated with HHV-6 reactivation was even reported.
Many other disorders are reported in association with EED, but most of them in only a few cases, making the establishment of a causative relationship doubtful. Thus, EED has been reported to be associated with many autoimmune disorders, such as rheumatoid arthritis [18, 19], celiac disease [20, 21], primary Sjögren syndrome [22], systemic lupus erythematosus [23], or antiphospholipid antibodies [24, 25], as well as inflammatory bowel disease [26] and solid neoplasms [1, 15].
Our patient had a history of type 2 diabetes mellitus and chronic obstructive pulmonary disease. We think that this association is rather fortuitous since both diseases are frequent and their pathogenesis does not seem related to the pathogenesis of EED.
However, because EED may precede serious hematologic diseases, we cannot confirm that this case is an idiopathic case until after several years of monitoring, despite the favorable response to treatment.
References
1. Wilkinson SM, English JSC, Smith NP, Wilson-Jones E, Winkelmann RK. Erythema elevatum diutinum: a clinicopathological study. Clin Exp Dermatol 1992;17:87-93. [PubMed]2. Ly H, Black MM. Atypical presentation of erythema elevatum diutinum. Australas J Dermatol 2005; 46:44-6. [PubMed]
3. Shanks JH, Banerjee SS, Bishop PW, Pearson JM, Eyden BP. Nodular Erythema elevatum diutinum mimicking cutaneous neoplasms. Histopathology 1997; 31:91-6. [PubMed]
4. Devillierre M, Verola O, Rybojad M. Pseudoneoplastic lesion of erythema elevatum diutinum. Ann Dermatol Venereol 2008;135:575-9. [PubMed]
5. Dronda F, Gonzalez-lopez A, Lecona MC. Erythema elevatum diutinum in human immunodeficiency virus-infected patients - report of a case and review of the literature. Clin Exp Dermatol 1996;21: 222-5. [PubMed]
6. Gibson LE, El-Azhary RA. Erythema Elevatum Diutinum. Clin Dermatol 2000;18:295-9. [PubMed]
7. High WA, Hoang MP, Stevens K, Cockerell CJ. Late-stage nodular erythema elevatum diutinum. J Am Acad Dermatol 2003;49:764-7. [PubMed]
8. Yiannias JA, EI-Azhary RA, Gibson LE. Erythema elevatum diutinum: A clinical and histopathological study of 13 patients. J Am Acad Dermatol 1992;26:38-44. [PubMed]
9. Arehimanditis AJ, Fertakis A, Alegakis G. Erythema elevatum diutinum and IgA myeloma: an interesting association. Br Med J 1977;2:613-4. [PubMed]
10. Hatzitolios A, Tzellos TG, Savopoulos C et al. Erythema elevatum diutinum with rare distribution as a first clinical sign of non-Hodgkin’s lymphoma: A novel association? J Dermatol 2008;35:297-300. [PubMed]
11. Delaporte E, Alfandari S, Fenaux P, Piette F, Bergoend H. Erythema elevatum diutinum and chronic lymphocytic leukaemia. Clin Exp Dermatol 1994;19:188-9. [PubMed]
12. Miyagawa S, Kitamura W, Morita K, Saishin M, Shirai T. Association of hyperimmunoglobulinaemia D syndrome with erythema elevatum diutinum. Br J Dermatol 1993; 128:572-4. [PubMed]
13. Futei Y, Konohana I. A case of erythema elevatum diutinum associated with B-cell lymphoma: a rare distribution involving palms, soles and nails. Br J Dermatol 2000;142:116-9. [PubMed]
14. Liu T, Chen I, Lin T, Lee JY, Kirn D, Tsao C. Erythema elevatum diutinum as a paraneoplastic syndrome in a patient with pulmonary lymphoepithelioma-like carcinoma. Lung Cancer 2009;63: 151-3.
15. Yilmaz F, Araç M, Çiftçioglu MA, Yilmaz E. A case of erythema elevatum diutinum associated with breast carcinoma. Int J Dermatol 2005;44:948-50. [PubMed]
16. Muratori S, Carrera C, Gorani A, Alessi E. Erythema elevatum diutinum and HIV infection: a report of five cases. Br J Dermatol 1999;141:335-8. [PubMed]
17. Rover PA, Bittencourt C, Discacciati MP, Zaniboni MC, Fávaro Arruda LH, Cintra ML. Erythema elevatum diutinum as a first clinical manifestation for diagnosing HIV infection: case history. Sao Paulo Med J 2005;123:201-3. [PubMed]
18. Collier PM, Neill SM, Branfoot AC, Staughton V. Erythema elevatum diutinum - a solitary lesion in a patient with rheumatoid arthritis. Clin Exp Dermatol 1990;15:394-5. [PubMed]
19. Muscardin LM, Cota C, Amorosi B, Ferraro C. Erythema elevatum diutinum in the spectrum of palisaded neutrophilic granulomatous dermatitis: description of a case with rheumatoid arthritis. J Eur Acad Dermatol Venereol 2007;21:104-43. [PubMed]
20. Kwon JL, Sigal AC, Bossenbroek NM. Erythema elevatum diutinum in association with celiac disease. Int J Dermatol 2009;48:787-9. [PubMed]
21. Rodriguez-Serna M, Fortea JM, Perez A, et al. Erythema elevatum diutinum associated with celiac disease: response to a gluten-free diet. Pediatr Dermatol 1993;10:125-8. [PubMed]
22. Shimizu S, Nakamura Y, Togawa Y, Kamada N, Kambe, Matsue H. Erythema elevatum diutinum with primary Sjögren syndrome associated with IgA antineutrophil cytoplasmic antibody. Br J Dermatol 2008; 159:733-75. [PubMed]
23. Hancox JG, Wallace CA, Sangueza OP, Graham GF. Erythema elevatum diutinum associated with lupus panniculitis in a patient with discoid lesions of chronic cutaneous lupus erythematosus. J Am Acad Dermatol 2004;50:652-3. [PubMed]
24. Yamamoto T, Nakamura S, Nishioka K. Erythema elevatum diutinum associated with Hashimoto’s thyroiditis and antiphospholipid antibodies. J Am Acad Dermatol 2005;165-6. [PubMed]
25. Lisi S, Mussi A, Muscardin L, Carducci M. A case of erythema elevatum diutinum associated with antiphospholipid antibodies. J Am Acad Dermatol 2003; 49:963-4. [PubMed]
26. Walker KD, Badame AJ. Erythema elevatum diutinum in a patient with Crohn's disease. J Am Acad Dermatol 1990;22:948-52. [PubMed]
© 2011 Dermatology Online Journal