Palisaded neutrophilic and granulomatous dermatitis
Published Web Location
https://doi.org/10.5070/D37qm0b0bsMain Content
Palisaded neutrophilic and granulomatous dermatitis
Alexandra Brecher MD PhD
Dermatology Online Journal 9(4): 1
From the Ronald O. Perelman Department of Dermatology, New York University
Abstract
A 46-year-old man with a history of systemic lupus erythematosus presented with a 6-month history of scaly, erythematous, tender nodules on his elbows and hands. Physical examination showed erythematous, umbilicated papules, with crusts on the elbows and the dorsa of the hands. Histopathologic examination demonstrated leukocytoclastic vasculitis with dense neutrophilic infiltrates and degenerated collagen, consistent with early palisaded neutrophilic and granulomatous dermatitis. The individual lesions were treated with intralesional glucocorticoid injections with some improvement.
Clinical summary
History.—A 46-year-old man presented to the Charles C. Harris Skin and Cancer Pavilion in August 2001 with a 6-month history of scaly, tender nodules on the elbows and on the dorsa of the hands. He had been admitted to Kings County Hospital 2 weeks previously with weakness, dizziness, and joint pain. A diagnosis of systemic lupus erythematosus was made, and he was started on prednisone and hydroxychloroquine. Past medical history includes visual impairment in the left eye and hearing loss in the left ear secondary to trauma and partial colectomy. Family history includes lupus erythematosus in his mother.
An initial biopsy specimen was interpreted as a palisaded neutrophilic and granulomatous dermatitis that is typically associated with collagen-vascular disease. Another biopsy specimen was obtained on a subsequent visit. Hydroxychloroquine and prednisone were continued, and intralesional glucocorticoids were used with some improvement.
Physical examination.—Multiple, erythematous nodules with scale were present on the dorsa of the hands and on the elbows. The knees and feet were clear.

|
|
| Figure 1 | Figure 2 |
|---|
Laboratory data.—The white-cell count was 7.1 x 109/L, hemoglobin 10.4 mg/dl, hematocrit 33.8 percent, platelet count 108 x 109/L, erythrocyte sedimentation rate 75 mm/hr, antinuclear antibody 1:10240 with speckled pattern, and anti-ds DNA 1:20. A basic metabolic panel, liver function tests, and urinalysis were normal.
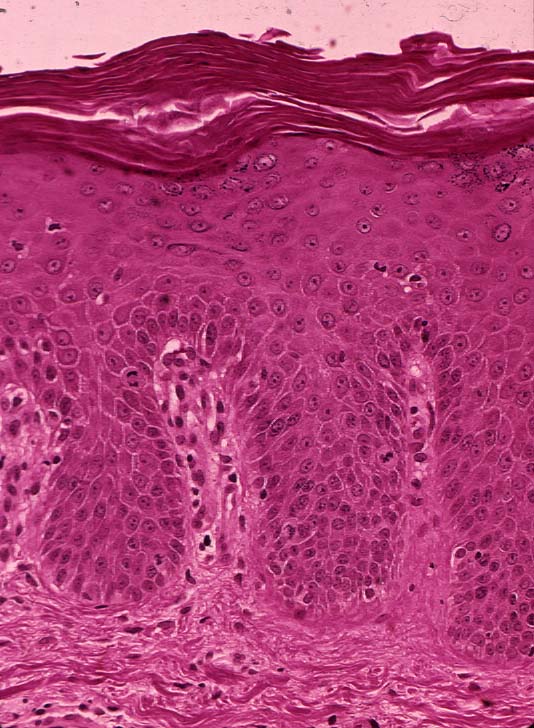
Histopathology.— There is focal leukocytoclastic vasculitis with adjacent degenerated collagen, nuclear dust surrounded by histiocytes, and fibrin deposits. There is a perivascular infiltrate of lymphocytes and macrophages. A periodic acid-Schiff stain for fungal organisms is negative. A Gram stain is negative for bacteria.
Diagnosis.—Palisaded neutrophilic and granulomatous dermatitis.
Comment
In 1984, Chu and associates coined the term palisaded neutrophilic and granulomatous dermatitis of immune-complex disease to describe those patients with lupus erythematosus, rheumatoid arthritis, and other diseases with immune complexes who develop symmetrical, papular lesions on the extremities. [1] Previously, the terms Churg-Strauss granuloma [2], cutaneous extravascular necrotizing granuloma, rheumatoid papules [3], superficial ulcerating rheumatoid necrobiosis, and interstitial granulomatous dermatitis with arthritis had been given to this entity.
The lesions of palisaded neutrophilic and granulomatous dermatitis are usually symmetrically distributed on the extremities and have smooth, ulcerated, or umbilicated surfaces. Histopathologic examination demonstrates a spectrum of changes that reflect the evolution of the lesions. Early lesions are characterized by leukocytoclastic vasculitis with dense neutrophilic infiltrates and degenerated collagen. Fully developed lesions show palisaded granulomas surrounding leukocytoclastic debris, fibrin, and altered collagen. Late-stage lesions are characterized by palisaded granulomas with dermal fibrosis and scant neutrophilic debris. Each stage of development elicits a different differential diagnosis.
The condition may persist for several months to 2 years. All patients had longstanding, active, collagen-vascular diseases that required medications such as oral prednisone, hydroxychloroquine, cyclosporine, cyclophosphamide, and nonsteroidal anti-inflammatory agents. Some of the lesions showed a good response to oral prednisone in doses of up to 20 mg daily; however, recurrences were common after treatment with prednisone was tapered.
References
1. Chu P, et al. The histopathologic spectrum of palisaded neutrophilic granulomatous dermatitis in patients with collagen vascular disease. Arch Dermatol 1994;130:1278.2. Finan MC, Winkelmann RK. The cutaneous extravascular necrotizing granuloma (Churg-Strauss granuloma) and systemic disease: a review of 27 cases. Medicine 1983;62:142.
3. Smith M, et al. Rheumatoid papules showing features of vasculitis and palisading granuloma. J Am Acad Dermatol 1989;20:348.
© 2003 Dermatology Online Journal