Orf parapoxvirus infection from a cat scratch
Published Web Location
https://doi.org/10.5070/D37kt9w318Main Content
Orf parapoxvirus infection from a cat scratch
Jonathan Frandsen, Mike Enslow, Anneli R Bowen MD
Dermatology Online Journal 17 (4): 9
University of Utah, Department of Dermatology, Salt Lake City, UtahAbstract
A 53-year-old woman presented with an enlarging, tender, ulcerated nodule on her dorsal hand after being scratched by a stray kitten. Histology was consistent with orf parapoxvirus infection. The lesion resolved without scarring after several weeks of treatment with imiquimod 5 percent cream. Orf is a zoonosis transmitted to humans from sheep and goats by direct contact or by fomites. Transmission by cat scratch has not been previously described in the literature.
Introduction
Orf virus infection, also known as ecthyma contagiousum or contagious pustular dermatitis, is caused by a prototypic member of the genus Parapoxvirus. Other members of this genus are pseudocowpox virus and bovine papular stomatitis virus in cattle, squirrel parapoxvirus, and parapoxvirus of red deer in New Zealand [1]. Orf is endemic to sheep and goats, but can also cause disease in humans [2].
Orf is transmitted by direct contact inoculation. Humans acquire the infection from contact with infected animals, carcasses, or contaminated, nonliving material [3, 4]. Cases of orf are almost exclusively reported in association with recent encounters with sheep or goats. However, transmission of the virus from deer to humans has been reported [5]. Orf is generally a benign, self-limited condition that regresses in 6 to 8 weeks without treatment [6]. It should be noted, however, that in immunocompromised individuals serious disease can develop [7].
We report a case in which an individual with no direct exposure to sheep, goats, or deer developed orf in association with a cat scratch.
Case report
 |
| Figure 1 |
|---|
| Figure 1. Farms near patient’s home |
A 53-year-old woman with a history of psoriasis, who was on 25 mg/week of methotrexate, presented to her primary care physician four weeks after being scratched by a stray kitten. She did not report ulcerating lesions on the kitten’s mouth or feet. The patient works in an office and lives in a farming community 20 miles south east of Salt Lake City, Utah. She denied any direct contact with cattle, sheep, goats, or deer, although these animals live in farmland and mountains near her home (Figure 1).
 |  |
| Figure 2a | Figure 2b |
|---|---|
| Figure 2a. Ulcerating, edematous nodule at site of stray cat scratch sustained four weeks prior to presentation. Figure 2b.The same area demonstrating complete resolution 10 weeks later following daily application of imiquimod 5 percent cream. | |
At the scratch site, she developed a painful blister that eventually ulcerated (Figure 2). She was treated with azithromycin and trimethoprim/sulfamethoxazole, but the lesion worsened. Culture of a skin swab grew normal skin flora. Bartonella serologies were negative. She was referred to the dermatology department where a skin biopsy was performed.
 |  |
| Figure 3a | Figure 3b |
|---|---|
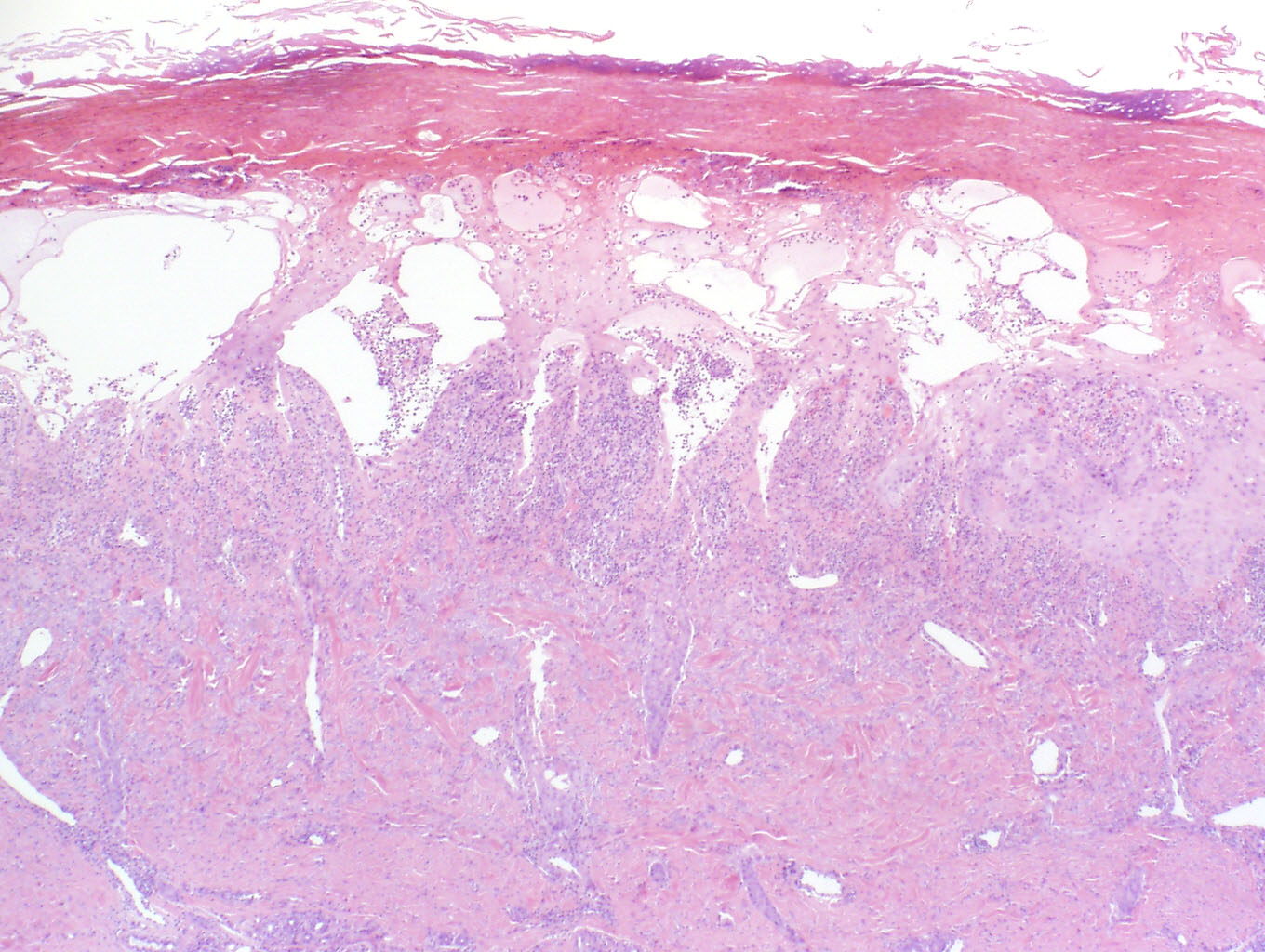
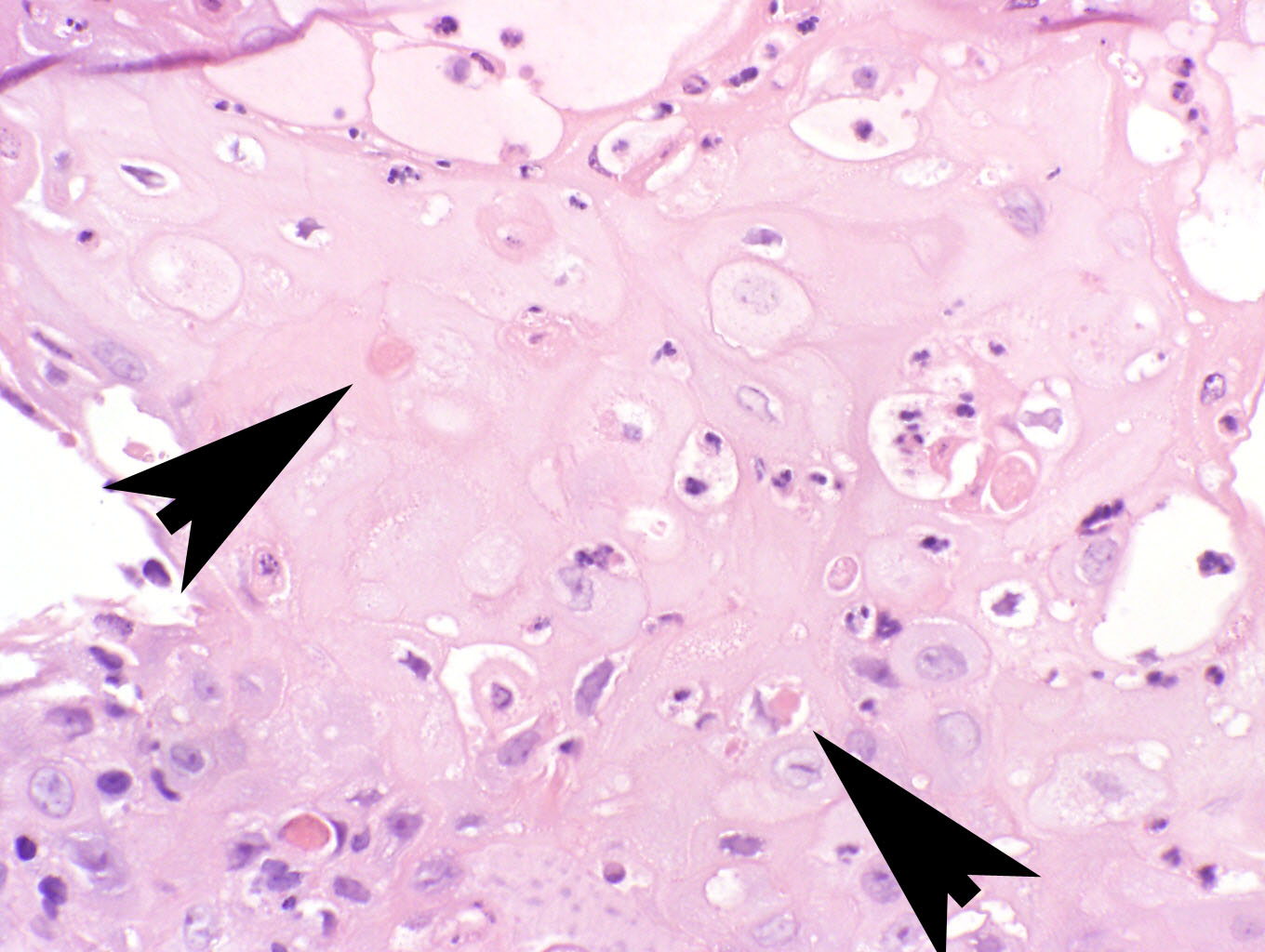
| Figure 3a. A biopsy from the periphery of the lesion in Figure 2A shows ballooning degeneration, spongiosis, and superficial
necrosis of the epidermis. Figure 3b. Eosinophilic, intracytoplasmic viral inclusions characteristic of parapoxvirus infection (arrows). | |
Biopsy revealed prominent epidermal spongiosis, ballooning degeneration of keratinocytes with subcorneal vesiculation, and a mixed inflammatory infiltrate of lymphocytes, histiocytes, and neutrophils (Figure 3). Keratinocytes demonstrated enlarged, glassy cytoplasms, prominent nuclei, and scattered single necrotic cells. Numerous eosinophilic cytoplasmic inclusions were present, characteristic of parapoxvirus infection (Figure 3). Both milker’s nodule and orf are in the histopathological differential diagnosis and have similar clinical behavior. Because milker’s nodules are smaller and less likely to ulcerate than orf, we assume our patient had orf, although the specific viral type could not be identified via PCR or immunohistochemistry performed on serum crust and paraffin embedded tissue (performed at the Center for Disease Control, Atlanta, Georgia).
Orf is a self-limited process. However, because the patient was immunosuppressed on methotrexate she was treated with imiquimod 5 percent cream daily. After 10 weeks, the lesion had completely healed without scar (Figure 2). The patient was subsequently restarted on her psoriatic medications and has not had a recurrence to date.
Discussion
The orf virus has been extensively investigated in recent years owing to its zoonotic importance and ability to cross infect a variety of other species. To our knowledge, orf transmission by cat scratch has not been previously reported, though transmission by fomites including sheep harnesses, burrs in sheep wool [3], and fences is well known.
Orf usually manifests on the hands, but unusual locations have been described including the nose [8], scalp [9], axilla [10], buttocks, and genitals [11]. Symptoms include vesicular or necrotic skin lesions, pain, pruritis, lymphangitis, axillary lymphadenitis, and rarely fever or malaise [6]. Incubation time ranges from a few days to 4 weeks. Characteristic histopathology includes epidermal ballooning degeneration with subcorneal vesiculation and a mixed inflammatory cell response of lymphocytes, histiocytes, and neutrophils. Orf histology is nearly identical to that of milker’s nodule.
The clinical differential diagnosis of ulcerating nodules of the hands includes cutaneous anthrax, other parapoxvirus infection such as milker’s nodule, tularemia, and Sweet syndrome.
Infectious diseases are rarely transmitted by cat scratch. The most well known is cat scratch disease caused by Bartonella henselae. Infectious diseases known to spread by cat to human contact are more numerous and include, among others: campylobacteriosis, plague, salmonellosis, dermatophytosis, leptospirosis, dipylidium caninum (dog and cat tapeworm), toxoplasmosis, dirofilariasis, and rabies [12]. Interestingly, orf affecting the feet of cats in rural areas has been described [13] and provides a precedent for cats to carry parapoxvirus on their extremities, as suspected in our case.
Parapoxvirus infection remains an active clinical entity in North America in the twenty-first century, with fomites playing an important role in transmission. Parapoxvirus infection such as orf or milker’s nodule is an important entity to consider when dealing with enlarging, weaping, ulcerative lesions, especially of the extremities. Clinicians must keep this in mind even in patients without the typical exposure history. In addition to the classic setting in farmers, animal handlers and veterinarians, those who frequent petting zoos, those who live or work in rural areas, or those whose household pets roam in rural areas may be affected.
References
1. Hosamani M Bhanuprakash V, Scagliarini A, Singh RK. Comparative sequence analysis of major envelope protein gene (B2L) of Indian orf viruses isolated from sheep and goats. Vet Microbiol. 2006 Sep 10;116(4):317-24. [PubMed]2. Paiba GA, Thomas DR, Morgan KL, Bennett M, Salmon RL, Chalmers R, Kench SM, Coleman TJ, Meadows D, Morgan-Capner P, Softley P, Sillis M, Green LE. Orf (contagious pustular dermatitis) in farmworkers: prevalence and risk factors in three areas of England. Vet Rec. 1999 Jul 3;145(1):7-11. [PubMed]
3. Centers for Disease Control and Prevention (CDC). Orf virus infection in humans- New York, Illinois, California, and Tennessee, 2004-2005. MMWR Morb Mortal Wkly Rep, 2006. 55(3): p. 65-8.
4. Hosamani M, Scagliarini A, Bhanuprakash V, McInnes CJ, Singh RK. Orf: an update on current research and future perspectives. Expert Rev Anti Infect Ther. 2009 Sep;7(7):879-93. [PubMed]
5. Kuhl JT, Huerter CJ, Hashish H. A case of human orf contracted from a deer. Cutis. 2003 Apr;71(4):288-90. [PubMed]
6. Erbağci Z, Erbağci I, Almila Tuncel A. Rapid improvement of human orf (ecthyma contagiosum) with topical imiquimod cream: report of four complicated cases. J Dermatolog Treat. 2005;16(5-6):353-6. [PubMed]
7. Ara M, Zaballos P, Sánchez M, Querol I, Zubiri ML, Simal E, Hörndler C. Giant and recurrent orf virus infection in a renal transplant recipient treated with imiquimod. Am Acad Dermatol. 2008 Feb;58(2 Suppl):S39-40. [PubMed]
8. Maki A Jr, Hinsberg A, Percheson P, Marshall DG. Orf: contagious pustular dermatitis. CMAJ. 1988 Nov 15;139(10):971-2. [PubMed]
9. Glass J, Ghali FE, Sinkre P, Ricotti CA, Cockerell CJ. Acute onset of erythematous scalp nodules in a child. Arch Dermatol. 2009 Sep;145(9):1053-8. [PubMed]
10. Weide B, Metzler G, Eigentler TK, Fehrenbacher B, Sönnichsen K, Garbe C. Inflammatory nodules around the axilla: an uncommon localization of orf virus infection. Clin Exp Dermatol. 2009 Mar;34(2):240-2. [PubMed]
11. Kandemir H, Ciftcioglu MA, Yilmaz E. Genital orf. Eur J Dermatol. 2008 Jul-Aug;18(4):460-1. [PubMed]
12. Elliot DL, Tolle SW, Goldberg L, Miller JB. Pet-associated illness. N Engl J Med. 1985 Oct 17;313(16):985-95. [PubMed]
13. Fairley RA, Whelan EM, Pesavento PA, Mercer AA., Recurrent localised cutaneous parapoxvirus infection in three cats. N Z Vet J. 2008 Aug;56(4):196-201. [PubMed]
© 2011 Dermatology Online Journal