Ulerythema ophryogenes and Noonan syndrome

Main Content
Ulerythema ophryogenes and Noonan syndrome
Jacqueline A Guidry MD, Adam Rees MD, Audrey J Chan MD, Fareesa Shuja MD, Sylvia Hsu MD
Dermatology Online Journal 19 (2): 14
Baylor College of Medicine, Department of Dermatology, Houston, TexasAbstract
We describe a patient with Noonan syndrome (NS) presenting with ulerythema ophrygenes (UO) – an association initially suggested in a single case series of five patients by Pierini and Pierini in 1979. Recognition of the association of UO with NS by pediatric dermatologists is important because of the high incidence of cardiovascular anomalies in NS. Therefore, in infants and children presenting with UO, clinicians should maintain a high index of suspicion for NS and refer for further workup.
Case report
A 21-month-old male with Noonan syndrome (NS) was sent for dermatologic evaluation. On physical exam, he was noted to have follicule-based hyperkeratotic papules on the trunk and extremities and follicule-based erythematous papules along the eyebrows in association with cicatricial madarosis. This finding is consistent with ulerythema ophrygenes (UO – also called keratosis pilaris atrophicans faciei). The patient was also noted to have low-set ears and other facial characteristics consistent with NS (hypertelorism, downward sloping palpebral fissures, depressed nasal bridge, micrognathia). He was recently diagnosed with hypertrophic cardiomyopathy likely related to pulmonary stenosis – the most common cardiac anomaly described in NS.
 |  |
| Figure 1 | Figure 2 |
|---|---|
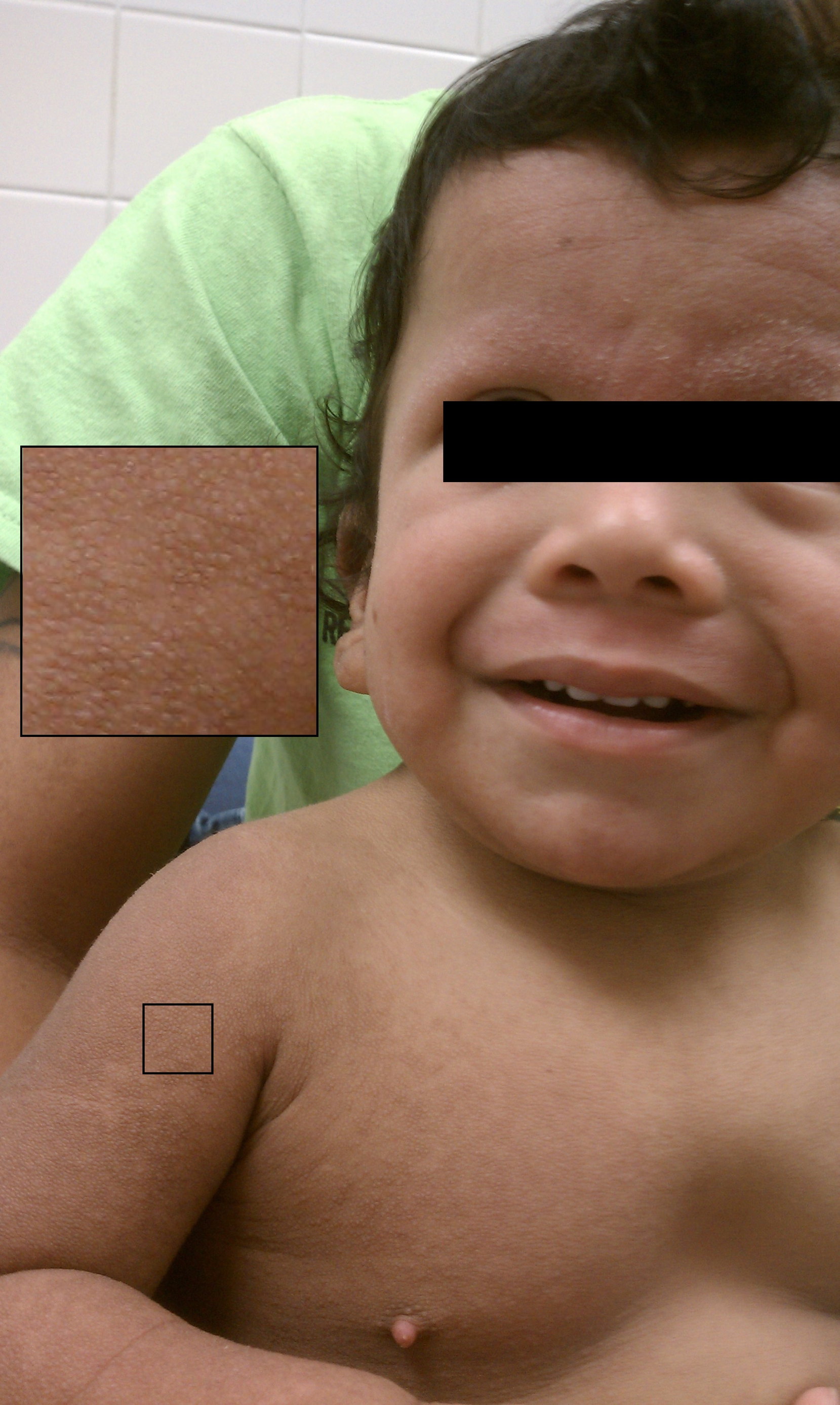
| Figure 1. Patient with Noonan syndrome and ulerythema ophryogenes. Note the follicule-based papules involving the eyebrows. Figure 2. Keratotic follicular papules on the arms. Also note the other characteristic features of Noonan syndrome including downward sloping palpebral fissures, low set ears, and pectus excavatum. | |
Discussion
Pierini and Pierini reported the first association of UO and NS in 1979. In a retrospective review of 9 cases of NS, 5 demonstrated UO. All 5 also had significant cardiac anomalies [1].
Noonan syndrome is a congenital disorder. The most common mode of inheritance is autosomal dominant with variable penetrance [2]. It is characterized by short stature, hypertelorism, ptosis, low-set ears, and cutaneous and cardiac anomalies. The cutaneous manifestations of NS include lymphedema, dystrophic nails, multiple pigmented nevi, curly hair, keloid formation, and UO. In UO, patients often present within several months of birth with follicule-based papules involving the eyebrows. The process may result in cicatricial alopecia of the eyebrow. There is often associated keratosis pilaris of the extensor arms, thighs, and buttocks [3].
Histologically, UO is characterized by a dystrophic or twisted hair inside a dilated follicle plugged with keratin. There may be associated inflammation and fibrosis postulated to be secondary to a blocked hair penetrating the follicular wall [3].
Since the initial case series, only 4 additional cases of UO in NS have been reported [2, 3, 4]. Despite this rarity, recognition of this association in the pediatric community is paramount because of the high incidence of cardiovascular anomalies (55–96%) in NS. Therefore infants or children with UO merit further workup for NS. Referrals to cardiology, genetics, and ophthalmology may be appropriate [5].
Conclusion
In pediatric patients presenting with UO, clinicians should carry a high index of suspicion for NS and refer for further workup if there are any suspicious findings.
References
1. Pierini DO, Pierini AM. Keratosis pilaris atrophicans faciei (ulerythema ophryogenes): a cutaneous marker in the Noonan syndrome. Br J Dermatol. 1979;100(4):409-16. [PubMed]2. Güleç AT, Karaduman A, Seçkin D. Noonan syndrome: a case with recurrent keloid formation. Cutis. 2001;67(4):315-6. [PubMed]
3. Snell JA, Mallory SB. Ulerythema ophryogenes in Noonan syndrome. Pediatr Dermatol. 1990;7(1):77-8. [PubMed]
4. Grob JJ, Laure M, Berge G, Taramasco M, Bore P, Benderitter T, Andrac L, Collet AM, Bonerandi JJ. [Cutaneous signs of Noonan's syndrome. Apropos of a case with ulerythema ophryogenes, disseminated pilar and sudoral keratosis and progressive alopecia]. Ann Dermatol Venereol. 1988;115(3):303-10.
5. Management of Noonan syndrome: A clinical guideline 2010. DYSCERNE – Noonan syndrome Guideline Development Group.
© 2013 Dermatology Online Journal