Treatment of crusted scabies with albendazole: A case report
Published Web Location
https://doi.org/10.5070/D375c8898zMain Content
Treatment of crusted scabies with albendazole: A case report
Thaer Douri MD, A Z Shawaf MD
Dermatology Online Journal 15 (10): 17
Ministry of Health, Syria-Hama. s-dori@scs-net.orgAbstract
Crusted scabies is a severe variant of scabies caused by the ectoparasite Sarcoptes scabiei. It is characterized by high mite burden, extensive hyperkeratotic scaling, crusted lesions, variable pruritus, generalized lymphadenopathy, erythroderma, and eosinophilia, in some cases. There is an increased incidence of crusted scabies, particularly among patients with HIV infection. We describe a 22-year-old Syrian immunocompetent female who had hyperkeratotic psoriasiform plaques and hyperkeratosis without itching. She was treated with oral albendazol and topical crotamiton with salicylic acid 5 percent.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|
A 22-year-old Syrian female had hyperkeratotic psoriasiform lesions of her axillae, anterior flexors, and the dorsum of her hands without itching (Figs. 1-4); the lesions had started two years previously and they were treated as psoriasis plaques without benefit.
 |  |
| Figure 3 | Figure 4 |
|---|
Her skin examination revealed large erythematous, hyperkeratotic, scaly plaques on the trunk, abdomen, and extremities, as well as numerous small erythematous papules with scattered excoriations around the umbilicus. Her head, as well as her palmoplantar surfaces and nails were free of any lesions.
Itching was absent. The patient had no history of significant medical problems and her general physical examination was normal. Laboratory exams were normal and HIV negative.
The presence of itching in the patient's family members made us concerned about a possible diagnosis of scabies.
 |  |
| Figure 5 | Figure 6 |
|---|
 |
| Figure 7 |
|---|
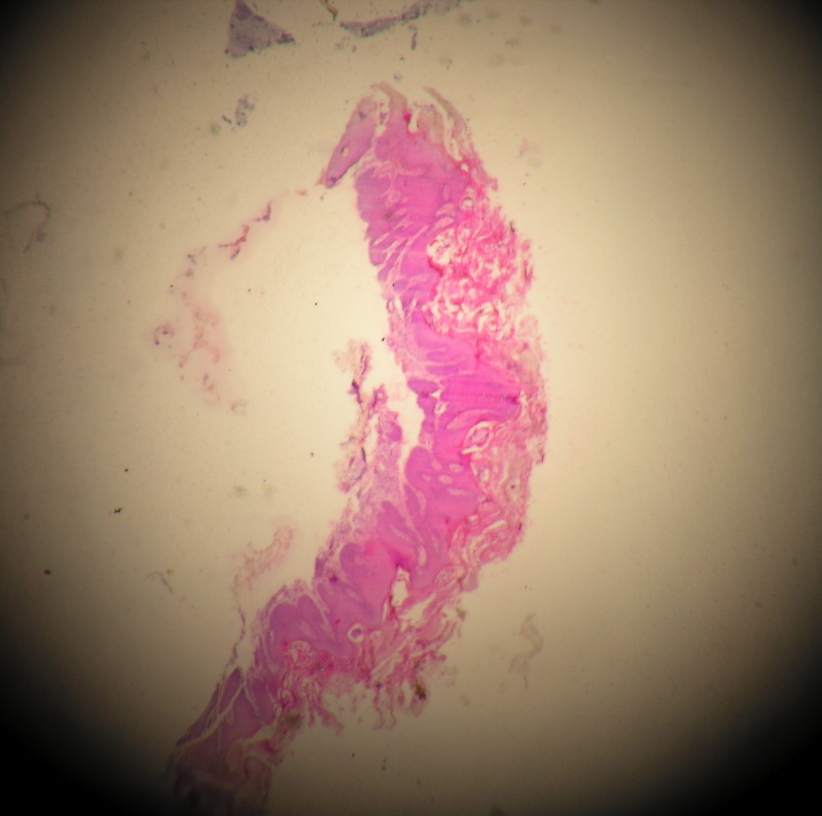
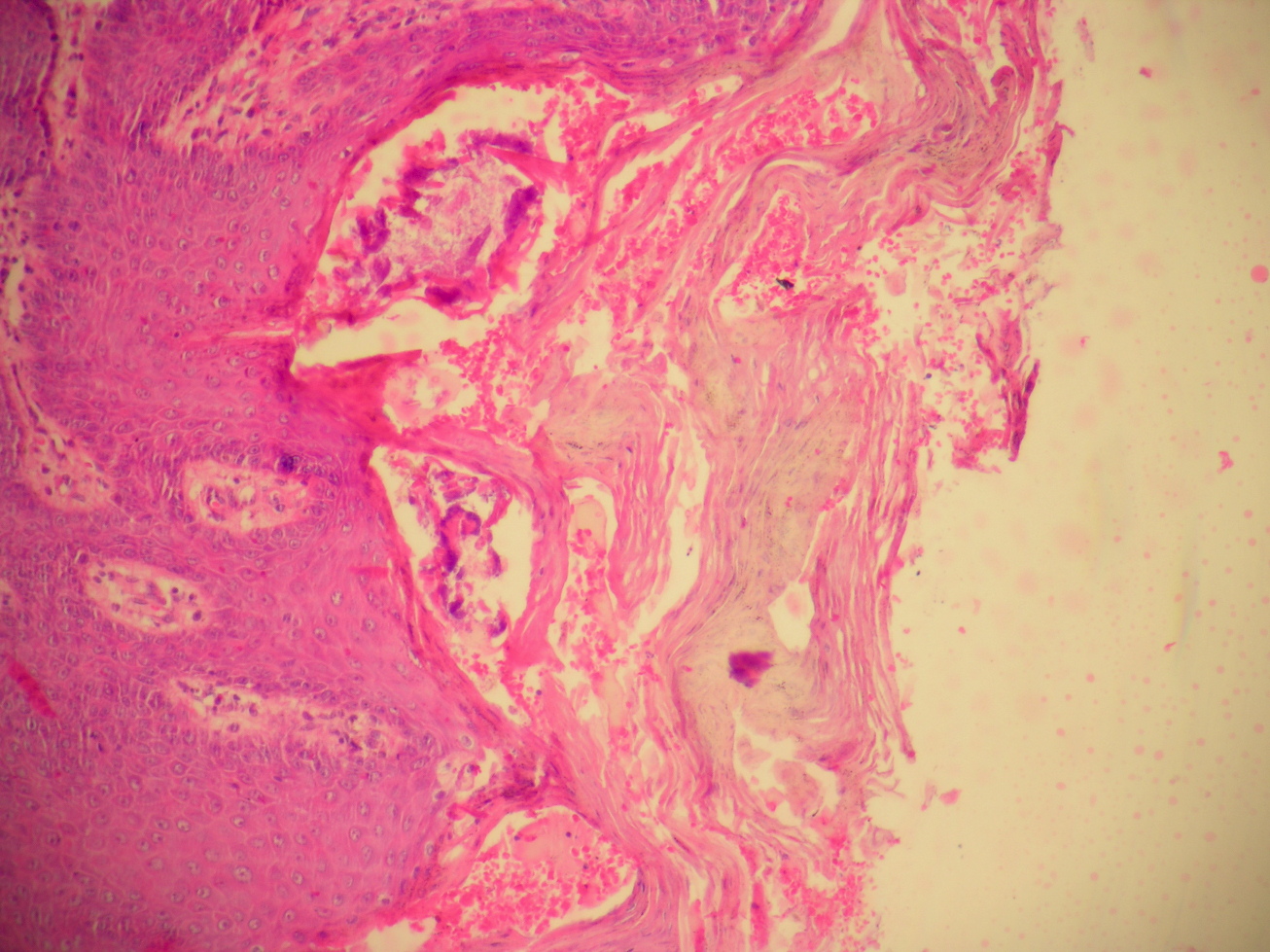
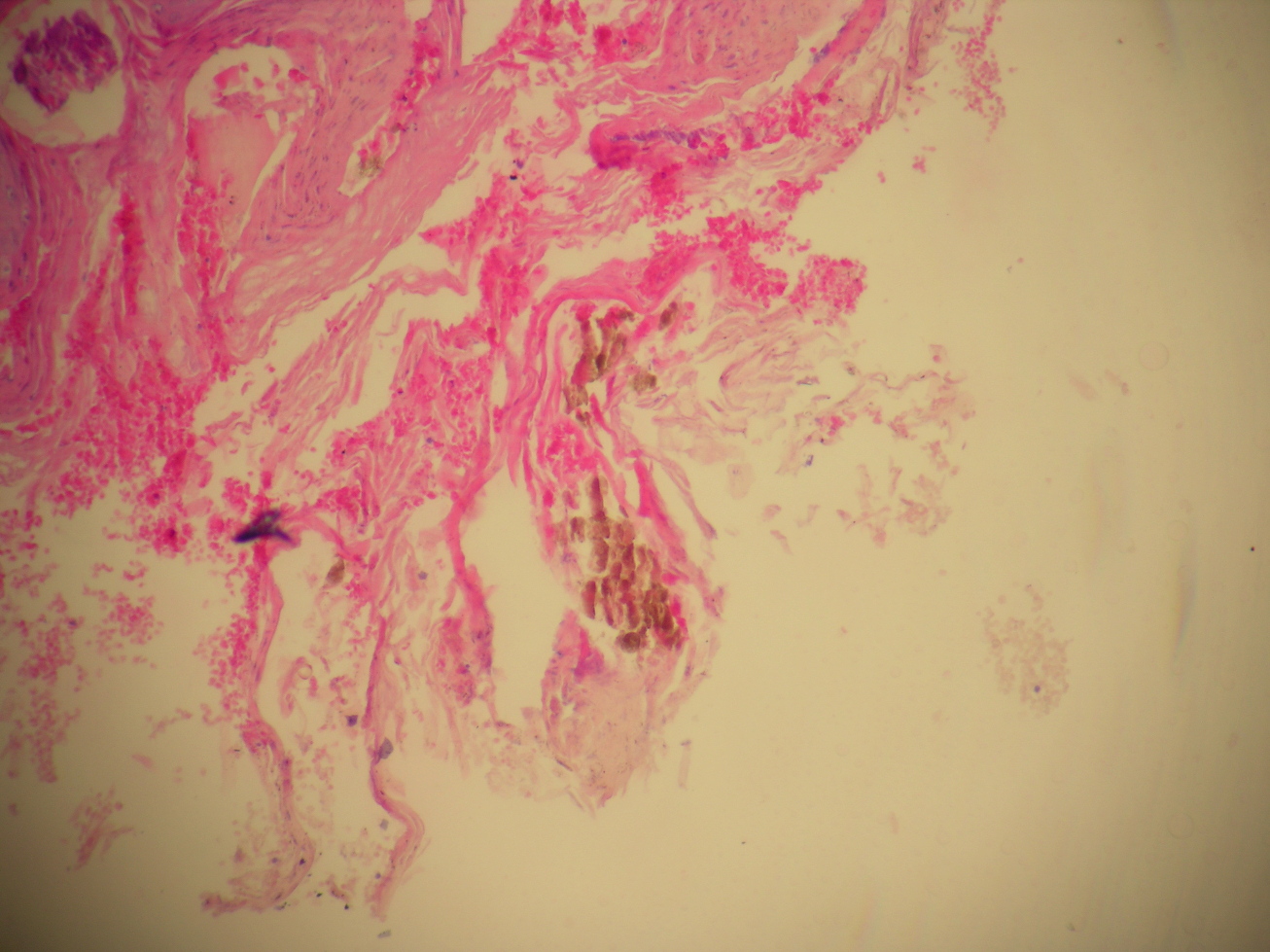
A biopsy was made: The epidermis shows marked hyperkeratosis, acanthosis, and burrows in the subcorneal layer containing female mites and feces (Figs. 5-7); the diagnosis of crusted scabies was made.
She was successfully treated with 800 mg of albendazole with fatty meals for 3 consecutive days and an application of a 5 percent salicylic acid in crotamiton twice daily for 1 week (Figs. 8 & 9). Her family was treated with benzyl benzoate 25 percent.
 |  |
| Figure 8 | Figure 9 |
|---|
Discussion
Crusted scabies is a severe variant of scabies caused by the ectoparasite Sarcoptes scabiei. The condition is characterized by high mite burden, extensive hyperkeratotic scales, crusted lesions, variable pruritus, generalized lymphadenopathy, erythroderma, and eosinophilia, in some cases. Crusted scabies may masquerade as hyperkeratotic eczema, psoriasis, Darier disease, and contact dermatitis [1].
In common scabies, there are few mites, probably because scratching destroys the burrows [1]. However, in crusted scabies there may be thousands or even millions of mites. The diagnosis is confirmed by examination of scrapings and biopsies that are teeming with mites and eggs [1].
Our patient, who apparently had not any underlying significant disease, lacked several features that are usually seen in crusted scabies. She also did not have any palmoplantar or subungual lesions.
Itching, which is the hallmark of scabies, was minimal or absent in this patient. It is generally believed that patients with crusted scabies do not itch. But, at least 50 percent of the patients have some degree of itching [2]. The itch, if present, diminishes with time. In our patient the itching was absent.
Treatment of crusted scabies can be very challenging because of various factors including the host's compromised immunity, the widespread nature of the eruption, the high mite burden, and the limited penetration of the topical agents into the hyperkeratotic lesions. Thus, the treatment of crusted scabies doesn't only include scabicidals, but also keratolytic agents to remove the thick crusts, which are a nidus for the mite. Removal of these crusts can be performed by employing a keratolytic agent such as 5-10 percent salicylic acid in petrolatumor 40 percent urea; soaking in a hot bath may also help. This may reduce the mite load and also enhances the efficacy of topical scabicidals [3]. Various topical agents and oral drugs used in the treatment of classical scabies are also used in treating crusted scabies [4] including topical sulfur compounds, benzyl benzoate, crotamiton, lindane, malathion, permethrin, and ivermectin [5].
Oral ivermectin has been proven to be very effective and is now considered as the treatment of choice for crusted scabies [4] and other resistant cases, but it is not available in Syria. Hence, we treat these patients with a daily dose of 800 mg of albendazole with fatty meals for 3 consecutive days and an application of 5 percent salicylic acid in crotamiton twice daily for 1 week.
Benzimidazoles (albendazole, fenbendazole, oxfenbendazole, mebendazole, and thiabendazole) are broad-spectrum antiparasitic agents used against a wide range of nematodes and cestodes. By binding to free B-tubulin, benzimidazoles inhibit the polymerization of tubulin and microtubule-dependant glucose uptake, leading to parasite death. These agents may additionally interfere with the synaptic transmission of parasites through a probable cholinergic effect [6]. Effectiveness of oral and topical thiabendazole against scabies has been pointed out in only a few reports since the 1960s [6, 7]; thiabendazole and the newer agent albendazole have been successfully used against pediculosis capitis [8, 9]. Drs. N. Ayoub, M. Merhy, and R. Tomb treated 2 cases of scabies successfully with a daily dose of 1000 mg of albendazole with fatty meals for 3 consecutive days and an application of a 5 percent salicylic acid ointment once daily for 1 week [10].
In conclusion, crusted scabies without involvement of palms, soles, and head is unusual. Our patient was also without subungual crusting, but exhibited the usual lack of pruritus. Crusted scabies can occur in apparently healthy persons. This possibility should be kept in mind in order to prevent misdiagnosis of this uncommon condition. Oral albendazol is safe and effective for treating scabies.
Acknowledgement: We thank reviewer Dr. Rasha Nabhan
References
1. Crusted scabies: alias Norwegian scabies. Parish LC, Lomholt G.Int J Dermatol. 1976 Dec;15:747-8. No abstract available. [PubMed]2. Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature.Roberts LJ, Huffam SE, Walton SF, Currie BJ. J Infect. 2005 Jun;50(5):375-81. [PubMed]
3. Hyperkeratotic plantar plaques in an HIV-positive patient. Crusted scabies, localized to the soles.Bitman LM, Rabinowitz AD. Arch Dermatol. 1998 Aug;134(8):1019, 1022-3. No abstract available. [PubMed]
4. Crusted scabies. Karthikeyan K. Indian J Dermatol Venereol Leprol. 2009 Jul-Aug;75(4):340-7. [PubMed]
5. Controlling scabies in institutional settings: a review of medications, treatment models, and implementation. Scheinfeld N. Am J Clin Dermatol. 2004;5(1):31-7. Review. [PubMed]
6. Allegre T, Cailleres S, Lota I, et al: Value of thiabendazole in scabies resistant to local treatment in HIV infected patients. Presse Med 1992;21: 1821-1822.
7. Hernandez-Perez E: Topically applied thiabendazole in the treatment of scabies. Arch Dermatol 1976; 112: 1400-1401.
8. Namazi MR: Treatment of pediculosis capitis with thiabendazole: a pilot study. Int J Dermatol 2003; 42: 973-976.
9. Akisu C, Delibas SB, Aksoy U: Albendazole: single or combination therapy with permethrin against pediculosis capitis. Pediatr Dermatol 2006; 23: 179-182.
10. Treatment of scabies with albendazole. Ayoub N, Merhy M, Tomb R. Dermatology. 2009;218(2):175. Epub 2008 Dec 6. No abstract available. [PubMed]
© 2009 Dermatology Online Journal