Worsening of contact dermatitis by oral hydroxyzine: A case report

Main Content
Worsening of contact dermatitis by oral hydroxyzine: A case report
Nianda Reid MD, Sunit Jariwala MD, Golda Hudes MD, Jason Fodeman MD, Elina Jerschow MD, David Rosenstreich MD
Dermatology Online Journal 19 (2): 4
Division of Allergy/Immunology, Montefiore Medical Center, Bronx, New YorkAbstract
Hydroxyzine is commonly used to treat pruritic skin lesions. Although rare, hydroxyzine can sometimes be linked to worsening dermatitis in patients who have sensitivities to phenothiazines and/or ethylenediamines. Herein we describe a patient who developed papulovesicular eruptions following the use of topical neomycin. Our patient’s contact dermatitis initially improved after the use of oral steroids. However, the patient’s skin condition was exacerbated by the continued use of hydroxyzine to treat her pruritus. Patch testing was positive at 48 hours for neomycin sulfate, ethylenediamine dihydrochloride, and p-phenylenediamine. Given the suspected cross-reactivity between hydroxyzine and ethylenediamine, hydroxyzine was discontinued and the patient’s cutaneous symptoms improved. In summary, physicians must be aware that oral hydroxyzine can worsen contact dermatitis in ethylenediamine-sensitive patients.
Introduction
Whereas the topical use of antihistamines has been known to induce hypersensitivity reactions, this is rarely the case for systemic antihistamines. Antihistamines are commonly used to treat pruritus in contact dermatitis. However, if there has already been topical sensitization, the systemic administration of antihistamines can cause a generalized exfoliative dermatitis [1]. This phenomenon has been demonstrated in a few case reports; such sensitivity has mostly been linked to phenothiazines and ethylenediamines [1, 2].
Ethylenediamine is an ingredient of aminophylline and cross reactions have been observed with some antihistamine and anti-nausea agents [4]. We report a case of worsening contact dermatitis following the administration of oral hydroxyzine in a patient presenting with contact dermatitis related to neomycin use. This case report highlights the importance of considering cross-reactions to hydroxyzine in patients with ethylenediamine sensitivity.
Case report
 |
| Figure 1 |
|---|
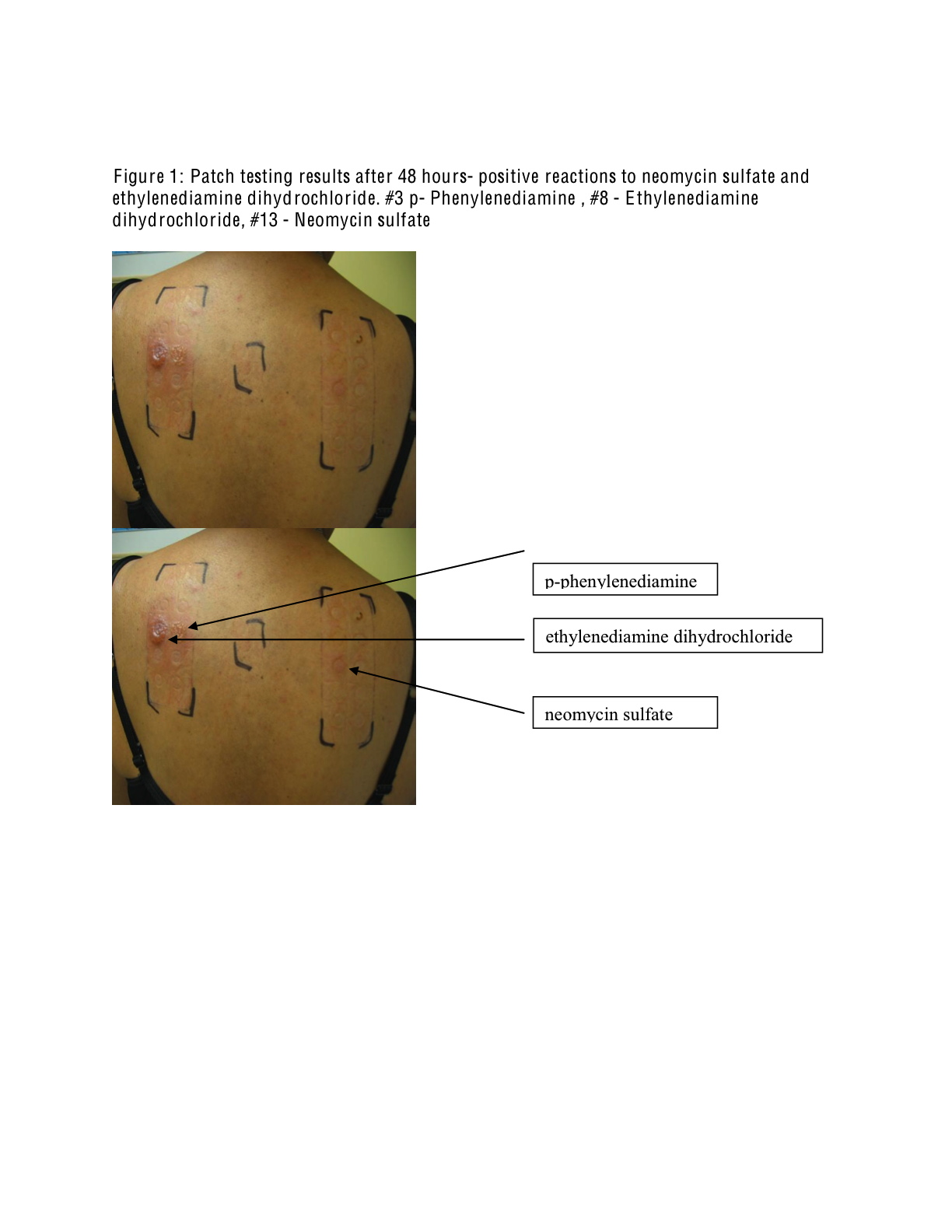
| Figure 1. Patch testing results after 48 hours- positive reactions to neomycin sulfate and ethylenediamine dihydrochloride. #3 p- Phenylenediamine , #8 - Ethylenediamine dihydrochloride, #13 - Neomycin sulfate |
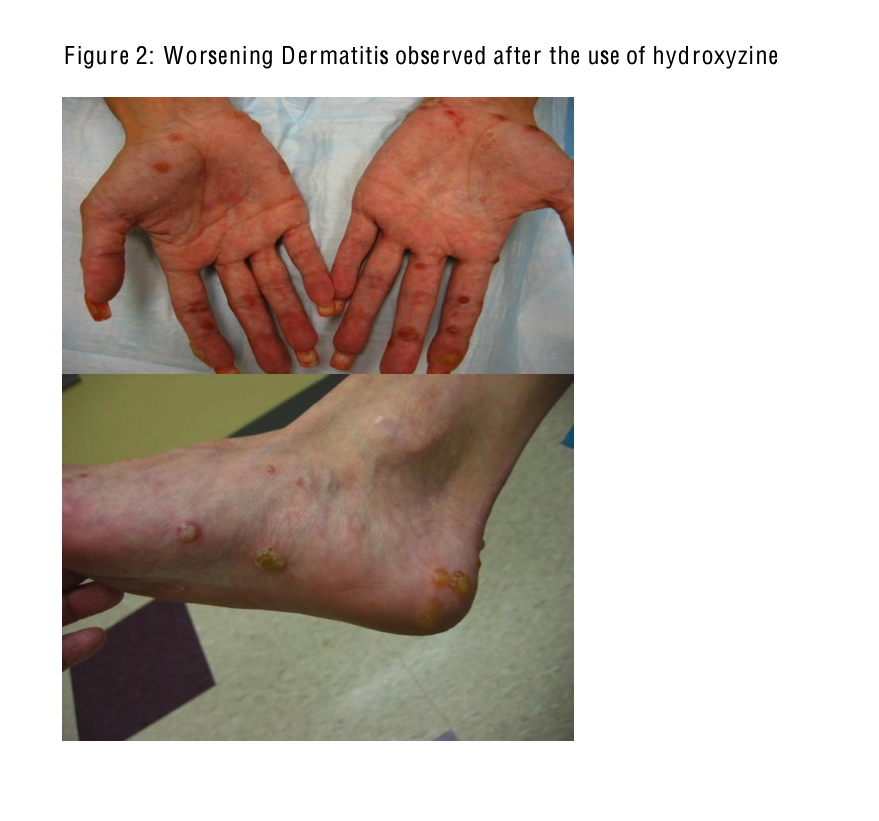
The patient is a 33-year-old female with a history of chronic stable asthma, chronic sinusitis, and allergic rhinitis who initially presented for the evaluation of suspected contact dermatitis. The patient first noticed a pruritic rash several days after the use of topical neomycin. She subsequently developed small and painful papulovesicular eruptions on her hands, elbows, shoulders, and feet. The lower extremity symptoms were so severe that the patient was unable to ambulate unassisted. The patient was initially evaluated in the emergency room and was treated with a five-day course of prednisone and daily hydroxyzine for her symptoms. She stopped using neomycin at that time and continued to take oral hydroxyzine one to two times per day for relief of her pruritus. The lesions were localized and resolved initially after the short course of prednisone. The patient continued to concurrently use hydroxyzine. When the oral prednisone course was discontinued, the patient experienced reappearance of the intensely pruritic skin lesions.
 |
| Figure 2 |
|---|
| Figure 2. Worsening Dermatitis observed after the use of hydroxyzine |
After two months of worsening symptoms on oral hydroxyzine, patch testing was performed. Patch testing was positive at 48 hours and 1 week for neomycin sulfate 20 percent, ethylenediamine dihydrochloride 1 percent, epoxy resin 1 percent, p-tert-butylphenol formaldehyde resin 1 percent, and nickel sulfate (Figure 1). Imidazolidinyl urea 2 percent was positive at 1 week. Because of the suspected cross-reactivity to hydroxyzine in the setting of ethylenediamine sensitivity, hydroxyzine was discontinued and the patient experienced rapid clinical improvement.
Discussion
Hydroxyzine hydrochlorides are categorized as nitrogen-linked ethylenediamine antihistamines and may rarely cause allergic reactions [3, 5]. Cutaneous reactions to hydroxyzine are related to the piperazine (diethylenediamine)-derived chemically related structures [6]. Ash et al describe a case of hydroxyzine causing worsening dermatitis in a patient with chronic eczema [5]. Reported sensitivities to H1 antagonists have been observed with phenothiazine-related compounds, but are somewhat rarely reported with the use of hydroxyzine [6]. In 2002, Tella et al reported a case of recurrent and exacerbating urticaria in a patient treated with cetirizine, an active metabolite of hydroxyzine [7].
In our patient, repeated provocation of her contact dermatitis while taking hydroxyzine led us to believe that hydroxyzine was the cause of her worsening cutaneous symptoms. In light of the published cross-reactivity between ethylenediamine and hydroxyzine chemical structures, hydroxyzine was suspected and later confirmed by patch testing. Because the patient had a positive patch test result to ethylenediamine, the hydroxyzine was discontinued and there was rapid clinical improvement.
Ethylenediamine-sensitive patients should be instructed to avoid systemic and topical exposures from antihistamines and other cross-reactive compounds. When treating a patient with contact dermatitis who presents with worsening symptoms after the use of antihistamines such as hydroxyzine, antihistamine-induced hypersensitivity must be considered and patch testing can be performed. Practitioners should be cautious about continued treatment of refractory contact dermatitis with antihistamines such as hydroxyzine until the etiology is clear.
References
1. Fisher AA. Antihistamine dermatitis. Cutis 1976, 18: 329. [PubMed]2. Michel M, Dompmartin A. Louvet S et al. Skin Reactions to Hydroxyzine. Contact Dermatitis 1997; 36: 147. [PubMed]
3. Fisher AA. Antihistamine dermatitis. In: Fisher AA, editor. Contact dermatitis. 5th ed. Philadelphia: Lea and Febiger, 2001. p. 185-231.
4. Price ML, Hall Smith SP. Allergy to Piperazine in a patient sensitive to ethylenediamine. Contact Dermatitis 194; 10: 120. [PubMed]
5. Ash S, Scheman AJ. Systemic contact dermatitis to hydroxyzine. Am J Contact Dermat. 1997 Mar;8(1):2-5. [PubMed]
6. Lew B-L, Haw C-R, Lee M-H. Cutaneous Drug Eruption from Certizine and Hydroxyzine. J Am Acad Dermatology 2004; 50: 953. [PubMed]
7. Tella R, Gaig P, Bartra J, Garcia-Ortega P. Urticaria to cetrizine. J Investig Allergol Clin Immunol 2002; 12(2):136-7. [PubMed]
© 2013 Dermatology Online Journal