Poliosis overlying a nevus with blue nevus features
Published Web Location
https://doi.org/10.5070/D36jt37011Main Content
Poliosis overlying a nevus with blue nevus features
Lorraine C Young MD1, Gregory S Van Dyke MD2, Shira Lipton MD3, Scott W Binder MD2
Dermatology Online Journal 14 (2): 20
1. David Geffen School of Medicine at the University of California, Los Angeles, Dermatology Division. lcyoung@mednet.ucla.edu2. David Geffen School of Medicine at the University of California, Los Angeles, Department of Pathology, Division of Dermatopathology 3. David Geffen School of Medicine at the University of California, Los Angeles
Abstract
Poliosis is a localized patch of gray or white hair. Because it can be seen with a variety of disorders and drugs, a full history and exam is indicated. Additionally, it can be associated with underlying benign and malignant tumors, necessitating histological identification. We review the lesions that are reported with poliosis. In addition, we will report a case of poliosis overlying an intradermal nevus with congenital as well as blue nevus features. To the best of our knowledge, blue nevus features associated with poliosis have not been previously described.
Clinical synopsis
 |
| Figure 1 |
|---|
| Figure 1: Violaceous nodule with overlying gray hairs on right scalp |
A 15-year-old girl presented with a congenital lesion on her scalp that was noted to be enlarging over the previous 2 months. Physical exam revealed a 6cm by 3cm soft, well demarcated and violaceous nodule on the right vertex of scalp. Surmounting the nodule were poorly demarcated gray hairs (Fig. 1). The remainder of the exam was normal.
The history of a recently enlarging congenital lesion prompted concern for a possible malignant transformation. Was this a congenital nevus transforming into a melanoma or a plexiform neurofibroma into a neurofibrosarcoma?
 |  |
| Figure 2 | Figure 3 |
|---|---|
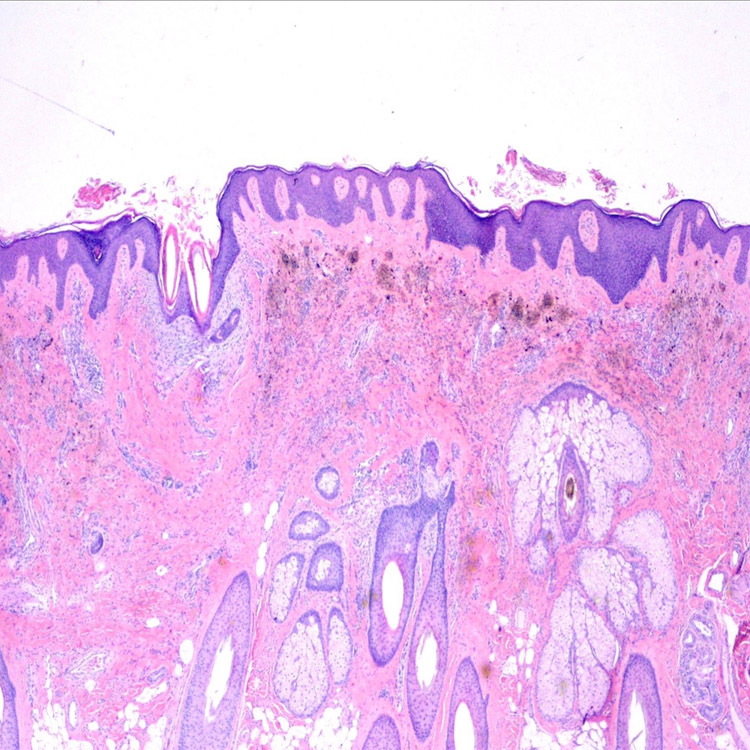
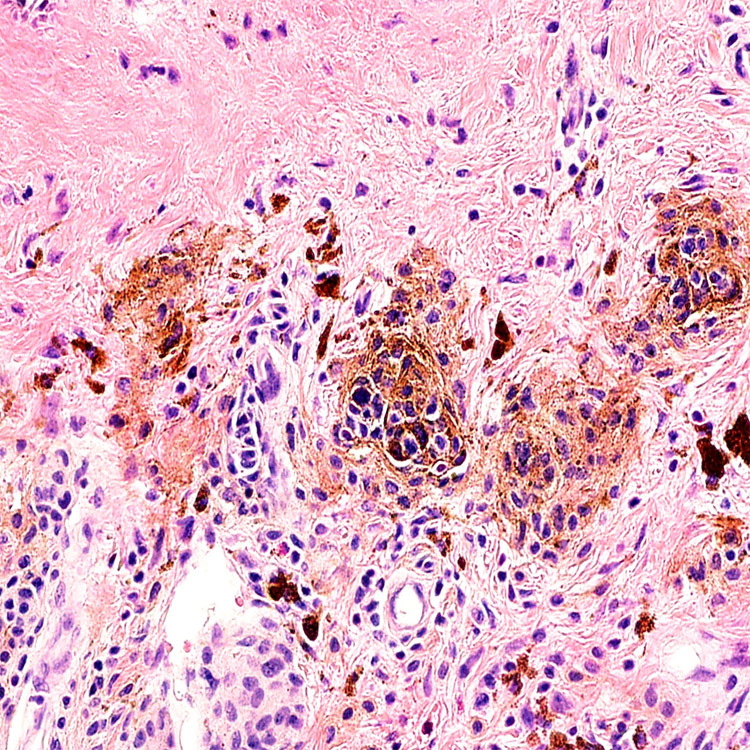
| Figure 2. Histological specimen shows nests of heavily pigmented melanocytes in the upper reticular dermis. Heavily pigmented
melanocytes with dendritic processes and pale-staining epithelioid melanocytes are present throughout the reticular dermis
between collagen bundles and surrounding adnexal structures. (Hematoxylin/eosin stain; original magnification: 10x). Figure 3. Magnification of Figure 2. (Hematoxylin/eosin stain; original magnification: 40x) | |
Prior to biopsy, a computerized axial tomography scan was performed to determine the size and extent of the nodule. A soft-tissue nodularity without evidence of osseous destruction was noted. Incisional and excisional biopsies revealed an intradermal melanocytic nevus with congenital as well as blue nevus features (Figs. 2 and 3). Histological specimens showed nests of heavily pigmented melanocytes in the upper reticular dermis. Heavily pigmented melanocytes with dendritic processes and pale-staining epithelioid melanocytes were present throughout the reticular dermis between collagen bundles and surrounding adnexal structures. Melanocytes with dendritic processes were highlighted with immunohistochemical staining with antibodies to S100 protein (Fig.4).
 |
| Figure 4 |
|---|
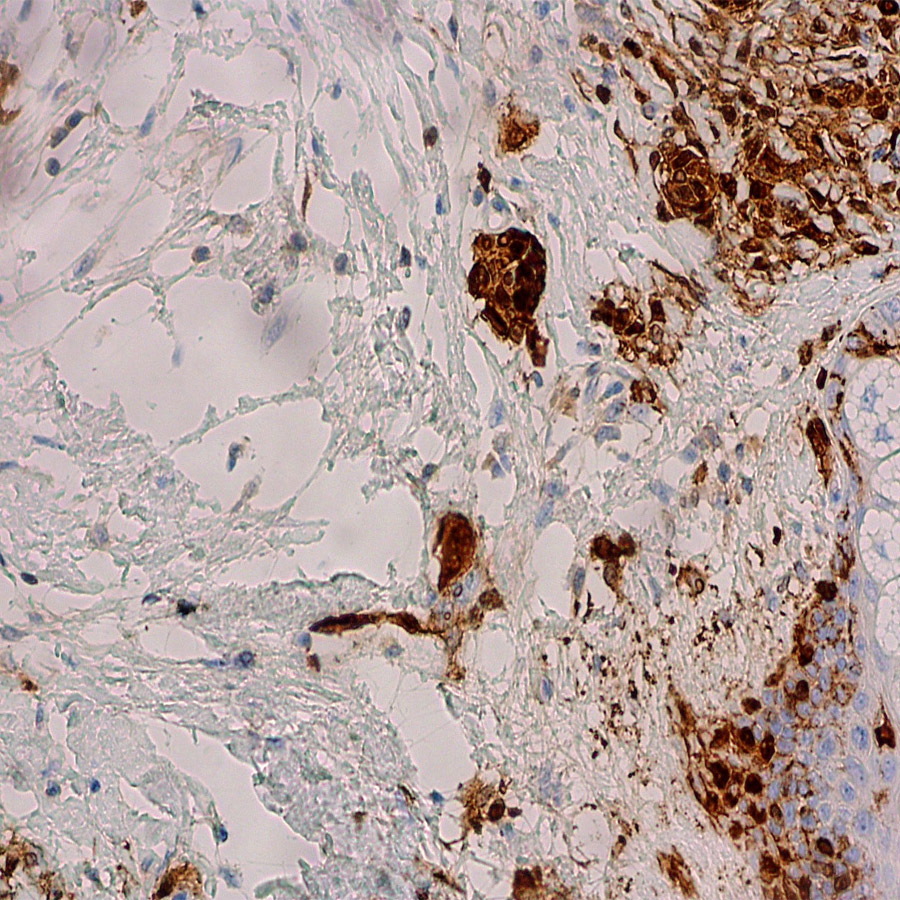
| Figure 4. Melanocytes with dendritic processes are highlighted with immunohistochemical staining with antibodies to S100 protein. (S100 stain; original magnification: 40x). |
Discussion
The literature regarding poliosis of the scalp has been dominated by case reports. Poliosis has been associated with a variety of diseases, drugs, and lesions. These include Marfan syndrome [1], Vogt-Koyanagi-Harada disease [2], sarcoidosis [3], herpes zoster [4], and alopecia areata [5]. Drugs, including chloroquine, cyclosporine, and topical prostaglandin F2α analogs [6] have also been reported to cause poliosis. In addition, poliosis can overlie lesions, including neurofibroma [7, 8, 9], giant congenital nevus [10], congenital intradermal nevus [11], nevus depigmentosus [12], halo nevus [13], nevus [14], and melanoma [15, 16].
Why this occurs is curious. Is it caused by destruction or dysfunction of melanocytes? Autoimmune and inflammatory diseases can damage melanocytes, and may explain why poliosis is associated with diseases such as alopecia areata, and herpes zoster, respectively. But what about poliosis associated with drugs? What about it overlying melanocytic lesions? Are melanocytes displaced? Do nevus cells take up melanin? If so, then what is the explanation for poliosis when it is associated with nonmelanocytic lesions such as neurofibromas? The pathogenesis is not known and is likely multifactorial.
Our patient presented at age 15 with an enlarging congenital lesion associated with a gray streak of hair. Previously reported scalp nodules associated with poliosis include both congenital and noncongenital nevi, halo nevi, melanoma, and neurofibroma. There are no prior reports, to the best of our knowledge, of poliosis overlying a nevus with blue nevus features.
Acknowledgement: We would like to acknowledge Scott McClennen, M.D., for taking the photo of the histology slide (Fig. 2).
References
1. Herman KL, Salman K, Rose LI. White forelock in Marfan's syndrome: an unusual association, with review of the literature. Cutis. 1991;48:82-84. PubMed2. Tsuruta D, Hamada T, Teramae J, Mito H, Ishii M. Inflammatory vitiligo in Vogt-Koyanagi-Harada disease. J Am Acad Dermatol. 2001;44:129-131. PubMed
3. Lett KS, Deane JS. Eyelash poliosis in association with sarcoidosis. Eye. 2005;19:1015-1017. PubMed
4. Wu JJ, Huang DB, Tyring SK. Postherpetic poliosis. Arch Dermatol. 2006;142:250-251. PubMed
5. Elston DM, Clayton AS, Meffert JJ, McCollough ML. Migratory poliosis: A forme fruste of alopecia areata? J Am Acad Dermatol. 2000;42:1076-1077. PubMed
6. Chen CS, Wells J, Craig JE. Topical prostaglandin F (2alpha) analog induced poliosis. Am J Optho. 2004;137:965-966. PubMed
7. Koplon BS, Shapiro L. Poliosis overlying a neurofibroma. Arch Dermatol. 1968;98:631-633. PubMed
8. Kwon IH, Cho JI, Lee SH, Lee JH, Cho KH, Kim JA, Moon SE. Poliosis circumscripta associated with neurofibroma. J Dermatol. 2005;32:446-449. PubMed
9. Heid E, Bekkali A, Lazrak B, Grosshans E. Neurofibroma, poliosis, and vitiligo. Ann Dermatol Venereol. 1978; 105:645-646. PubMed
10. Yosipovitch G, Feinmesser M, Mutalik S. Poliosis associated with a giant congenital nevus. Arch Dermatol. 1999;135:859-861. PubMed
11. Mendez B, Wood C. Poliosis in a scalp nodule: congenital intradermal nevus with poliosis. Arch Dermatol. 1993;129:1333-1336. PubMed
12. Dhar S, Kanwar AJ, Ghosh S. Leukotrichia in nevus depigmentosus. Pediatr Dermatol. 1993;10:198-199. PubMed
13. Fellman AC, Mehregan AH. Letter: Halo nevi of scalp with poliosis. Arch Dermatol. 1976;112:559. PubMed
14. Walker S, Lucke TW, Burden AD, Thomson J. Poliosis circumpscripta associated with scalp naevi: a report of four cases. Br J Dermatol. 1999;140:1182-1184. PubMed
15. Dunn CL, Harrington A, Benson PM, et al. Melanoma of the scalp presenting as poliosis circumscipta. Arch Dermatol. 1995;131:618-619. PubMed
16. Sober AJ, Haynes HA. Uveitis, poliosis, hypomelanosis, and alopecia in a patient with malignant melanoma. Arch Dermatol. 1978;114:439-441. PubMed
© 2008 Dermatology Online Journal