Acquired perforating disorder
Published Web Location
https://doi.org/10.5070/D368w0w9x9Main Content
Acquired perforating disorder
Olympia Kovich MD
Dermatology Online Journal 10 (3): 16
From the Ronald O. Perelman Department of Dermatology, New York University
Abstract
A 53-year-old man presented with asymptomatic, hyperkeratotic papules and hyperpigmented macules of the face and upper extremities. Treatment was initiated with topical tretinoin and intralesional glucocorticoids. Acquired perforating disorder is a disorder of keratinization that is associated with diabetes mellitus and uremia. Classic presentation involves hyperkeratotic papules with a central core, which occur most frequently on the lower extremities. Treatment includes topical tretinoin, glucocorticoids, keratolytics, systemic retinoids and glucocorticoids, and ultraviolet B phototherapy.
Clinical synopsis
History.—The patient is a 53-year-old African American man with a past medical history of hepatitis C virus, asthma, pancreatitis, diabetes mellitus, and chronic renal insufficiency, who has required hemodialysis since March 2002. A previous diagnosis of a perforating skin disease was based on biopsy specimens of the chest and back. He presented again in March, 2004, with a history of asymptomatic lesions on his face and upper extremities for one year. Treatment was initiated with tretinoin 0.05% cream daily and intralesional glucocorticoids.
Physical examination.—Localized to the face and upper extremities were multiple hyperkeratotic papules and hyperpigmented macules.

|

|
| Figure 1 | Figure 2 |
|---|
|
| Figure 3 |
|---|
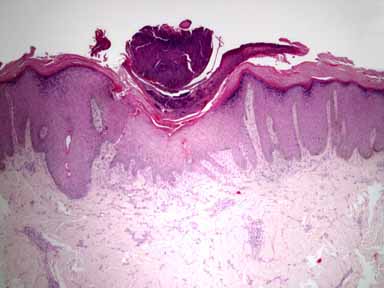
Histopathology.—There is an irregular, epidermal and epithelial hyperplasia with hypergranulosis. Centrally, there is a thick, hyperkeratotic and parakeratotic plug containing basophilic material that is embedded in an epidermal invagination.
Diagnosis.—Acquired perforating disorder.
Comment
Initially described by Kyrle in 1916 as hyperkeratosis follicularis et follicularis in cutem penetrans, acquired perforating disorder is one of a group of disorders characterized by the transepidermal elimination of dermal connective tissue. [1] This group of disorders includes elastosis perforans serpiginosa, reactive perforating collagenosis, perforating folliculitis, acquired perforating collagenosis, and Kyrle disease. Disagreement exists regarding whether Kyrle disease is distinct disorder or is a subtype of acquired perforating collagenosis.
Although the precise pathogenesis is unknown, acquired perforating collagenosis has been found to be associated with types I and II diabetes mellitus in as many as 90 percent of cases as well as with chronic renal disease. [2] One proposed mechanism involves increased levels of fibronectin, which is an adhesive glycoprotein that forms part of the extracellular matrix, in the sera and skin of patients with predisposing diseases (diabetes mellitus, uremia, and inborn errors of fibroblast synthesis, such as osteogenesis imperfecta and Marfan disease). [3] The authors propose that deposition of fibronectin may promote epithelial migration and proliferation and ultimately lead to transepidermal elimination, which is the hallmark of perforating disorders. [3]
The typical clinical presentation of this disorder is the presence of chronic, scattered, hyperkeratotic papules, which develop a central, cone-shaped plug. Although lesions usually spare the mucous membranes and acral regions, a few cases of ocular involvement have been reported. [4]
Histopathologic findings depend on the stage of evolution of the lesion. The histology may resemble any of the other perforating disorders, which has led to confusion concerning classification of acquired perforating disorder in the past. The dermal connective tissue eliminated in acquired perforating disorder is often amorphous degenerated material, which is not clearly identifiable as collagen or elastic fibers. [1] Treatment options include topical tretinoin, glucocorticoids, keratolytics, systemic retinoids, systemic glucocorticoids, and phototherapy. Narrow-band ultraviolet B phototherapy may be particularly effective for patients with this disorder because of the frequent concomitant uremic pruritus. [1]
References
1. Rapini, R. Perforating diseases. In Bolognia JL, et al., Eds. Dermatology. Mosby: London, 2003: 1497.2. Cunnigham SR, et al. Kyrle's Disease. J Am Acad Dermatol 1987; 16: 117.
3. Morgan MB, et al. Fibronectin and the extracellular matrix in the perforating disorders of the skin. Am J Dermatopathol 1998; 20: 147.
4. Alyahya GA, et al. Ocular changes in a case of Kyrle's disease: 20-year follow-up. Acta Ophthalmologica Scand 2000; 78:5 85.
© 2004 Dermatology Online Journal