Drug-induced linear IgA bullous dermatosis
Published Web Location
https://doi.org/10.5070/D3676552r9Main Content
Drug-induced linear IgA bullous dermatosis
Daniel Navi MD, Daniel J Michael MD PhD, Nasim Fazel MD DDS
Dermatology Online Journal 12 (5): 12
University of California Davis Department of Dermatology. nasim.fazel@ucdmc.ucdavis.eduAbstract
A 73-year-old man was admitted to the University of California Davis Medical Center for treatment of a pleural effusion and congestive heart failure. His hospital course was complicated by asymptomatic sustained ventricular tachycardia requiring placement of an implantable cardiac defibrillator. The patient was treated with vancomycin and cefazolin during the procedure. After 3 days he developed tense vesicles over the dorsal aspect of the hands. Perilesional skin biopsy showed subepidermal cleavage with a neutrophilic infiltrate. Direct immunofluorescence revealed granular IgA and C3 deposition along the dermal epidermal junction. A diagnosis of drug-induced linear IgA bullous dermatosis secondary to vancomycin was established. Linear IgA bullous dermatosis is a rare autoimmune blistering disorder with clinical features that can overlap with bullous pemphigoid and dermatitis herpetiformis. Drug-induced linear IgA bullous dermatosis is a less common variant that is correspondingly less well characterized. Although a variety of medications have been implicated, vancomycin is the most common associated drug.
Clinical Synopsis
A 73-year-old man was admitted to the University of California Davis Medical Center for treatment of a pleural effusion and congestive heart failure. His past medical history was significant for diabetes mellitus, hypertension, and peripheral vascular disease. Medications at the time of admission were metoprolol, lisinopril, omeprazole, aspirin, iron, and vitamin C.
He was started on carvedilol, lisinopril, and furosemide. On hospital day 4, he developed asymptomatic sustained ventricular tachycardia requiring placement of an implantable cardiac defibrillator. He was treated with vancomycin and cefazolin during the procedure. After the procedure spironolactone, amlodipine, and simvastatin were added.
On hospital day 7, he developed tense pruritic vesicles over the dorsal aspects of the hands. Over the course of a day, more lesions developed on his dorsal hands, wrists, and extensor forearms. Diphenhydramine was started to control the pruritus. A dermatology consult was requested. On exam he had clear yellow vesicles and small bullae on a pale erythematous bases, as well as erythematous boggy thin flat round papules on the dorsum of the hands, wrists, and on the forearms. A few linear superficial erosions were noted.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Tense vesicles on an erythematous base on the dorsal hand Figure 2. Tense vesicles and erythematous thin flat boggy papules on the extensor forearm | |
 |
| Figure 3 |
|---|
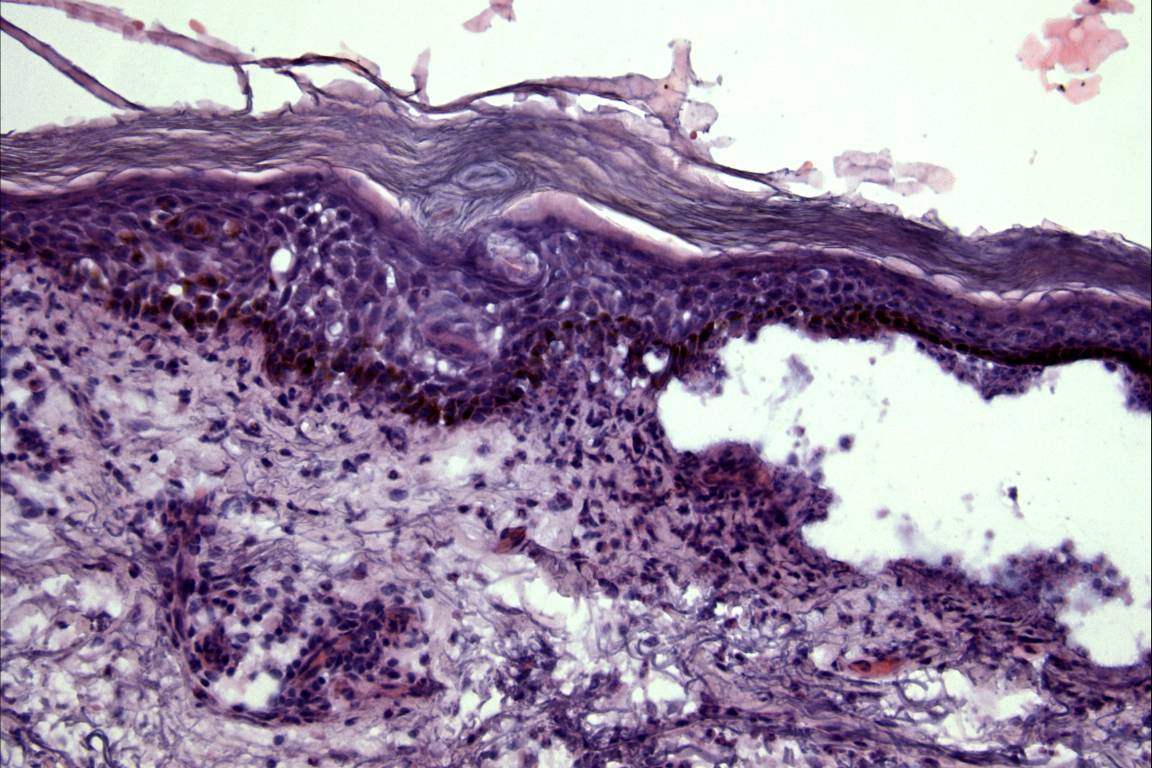
| Figure 3. Subepidermal clefting with an infiltrate consisting primarily of neutrophils (hematoxylin and eosin) |
A perilesional full-thickness biopsy was performed that showed subepidermal cleavage with a neutrophilic infiltrate. Direct immunofluorescence revealed granular IgA and C3 deposition along the dermal epidermal junction. There was no significant epidermal, junctional, or perivascular IgM, IgG, or fibrinogen deposition. A diagnosis of drug-induced linear IgA bullous dermatosis was established. The vancomycin was discontinued and the lesions completely resolved within 2 weeks.
Comment
Linear IgA bullous dermatosis (LAD) is a rare autoimmune blistering disorder characterized by subepidermal blistering with IgA deposition along the basement membrane zone. It was first distinguished from dermatitis herpetiformis (DH) in 1979 by Chorzelski [18]. The majority of LAD cases are idiopathic and may wax and wane over a course of years [19]. The clinical features of idiopathic LAD may overlap with other blistering disorders, such as bullous pemphigoid, dermatitis herpetiformis, and cicatricial pemphigoid [19]. There have been reports of patients with IgA and IgG antibody deposition consistent with an overlap between linear IgA bullous dermatosis and bullous pemphigoid [11, 12].
Although they are significantly less common, cases of drug-induced LAD have been reported [2]. In contrast to idiopathic LAD, drug-induced LAD develops within 1-15 days of the first dose of the inducing medication and resolves within 2 weeks of its discontinuation. Often the history helps to distinguish drug-induced LAD from other blistering disorders such as erythema multiforme and toxic epidermal necrolysis [3]. Within the drug-induced subset, vancomycin is the most commonly reported inducing agent [1, 2]. Cutaneous findings of drug-induced LAD, like idiopathic LAD, are also quite variable and include bullous, urticarial, erythematous, and targetoid erythema multiforme-like lesions often favoring the trunk, extremities, palms, soles, and sparing the head and neck [4].
The etiology of LAD is not fully understood. A heterogeneous group of antigens has been elucidated as targets in the idiopathic form of the disease. These antigenic targets are localized to the basement membrane zone (BMZ). Interestingly, the 97Kd ectodomain of the 180Kd bullous pemphigoid antigen and type-VII collagen, are two of the most commonly identified antigens, and may play a pathogenic role [5, 6, 7, 8]. Given the rare incidence of drug-induced LAD, far fewer studies have been able to characterize the target antigens involved in the drug-induced subset. Two studies have found antibodies to the 230kD antigen, the 97kD antigen, and type-VII collagen in non-vancomycin drug-induced LAD [1, 9] and one study described two patients with vancomycin-induced LAD with autoantibodies directed against BP180 and LAD 285 [7].
Histologically, LAD shows subepidermal blisters with an infiltrate primarily consisting of neutrophils. Direct immunofluorescence of perilesional skin usually shows deposition of IgA along the BMZ, usually in a homogenous linear pattern. Examples of granular linear deposition at the BMZ have also been identified [20]. In addition, IgG and C3 deposition at the BMZ are also found on occasion [13]. Serum assays and indirect immunofluorescence on monkey esophagus or salt-split human skin are usually negative, but there are reports of positive indirect immunofluorescence on the dermal side of salt-split human skin [10]. To our knowledge, only homogenous linear IgA deposition along the BMZ has been reported in vancomycin-induced linear IgA disease (VILAD). Here we report a case of drug-induced LAD with granular rather than linear deposition of both IgA and C3 along the dermal-epidermal junction. In addition to IgA deposition, linear deposition of C3 with weak deposition of IgG has also been reported in VILAD. There has been a report of a second-generation cephalosporin-inducing LAD, so, although it is significantly less likely, the role of cefazolin (a first generation cephalosporin) cannot be ruled out in our case.
Although the clinical, histological and immunofluorescence features of drug-induced LAD are indistinguishable from the idiopathic subtype, the history and course of drug-induced LAD helps to separate it from the more common idiopathic form. In contrast to idiopathic LAD, which is sporadic and carries considerable risk for persistence and scarring, drug-induced LAD is usually benign and transient. It generally occurs within 24 hours to 15 days following administration of the offending drug, with a mean onset of approximately 8 days [14]. The risk of VILAD is apparently not dose dependent and the severity of the reaction does not correlate with serum vancomycin levels [10, 13]. In our patient the blistering eruption occurred 2 days following the first dose of vancomycin. Such short latency has been seen in at least 2 other cases, in which the eruption occurred within 1 day of drug administration [11, 12]. Although the frequency of mucosal involvement in idiopathic LAD is as high as 80 percent [15], it was initially thought to be a rare occurrence in drug-induced LAD [16,17]. However, review of the recent literature suggests that mucosal involvement occurs in 40-45 percent of cases of drug-induced LAD [7,10].
Unlike the prolonged course of idiopathic LAD, which often requires medications both acutely and as maintenance therapy, nearly all patients with the drug-induced disease have spontaneous remission and clearance of immune deposits after withdrawal of the drug. Typically new lesions cease to form 24-72 hours after discontinuation of the offending agent and remaining lesions resolve within 2-7 weeks [14]. Dapsone and corticosteroids have been used in the treatment of VILAD however, the effect of these medications in disease resolution is unclear [3, 7]. Direct immunofluorescence study of perilesional skin should be performed in all cases of suspected VILAD to confirm the diagnosis and vancomycin should be promptly discontinued.
References
1. Wakelin SH, Allen J, Zhou S, Wojnarowska F. Drug-induced linear IgA disease with antibodies to collagen VII. Br J Dermatol. 1998 Feb;138(2):310-4. PubMed2. Nousari HC, Costarangos C, Anhalt GJ. Vancomycin-associated linear IgA bullous dermatosis. Ann Intern Med. 1998 Sep 15;129(6):507-8. No abstract available. PubMed
3. Waldman MA, Black DR, Callen JP. Vancomycin-induced linear IgA bullous disease presenting as toxic epidermal necrolysis. Clin Exp Dermatol. 2004 Nov;29(6):633-6. PubMed
4. Collier PM, Wojnarowska F. Drug-induced linear immunoglobulin A disease. Clin Dermatol. 1993 Oct-Dec;11(4):529-33. No abstract available. PubMed
5. Ishiko A, Shimizu H, Masunaga T, Yancey KB, Giudice GJ, Zone JJ, Nishikawa T. 97 kDA linear IgA bullous dermatosis antigen localizes in the lamina lucida between the NC16A and carboxyl terminal domains of the 180 kDa bullous pemphigoid antigen. J Invest Dermatol. 1998 Jul;111(1):93-6. PubMed
6. Marinkovich MP, Taylor TB, Keene DR, Burgeson RE, Zone JJ. LAD-1, the linear IgA bullous dermatosis autoantigen, is a novel 120-kDa anchoring filament protein synthesized by epidermal cells. J Invest Dermatol. 1996 Apr;106(4):734-8. Erratum in: J Invest Dermatol 1996 jun;106(6):1343. PubMed
7. Palmer RA, Ogg G, Allen J, Banerjee A, Ryatt KS, Ratnavel R, Wojnarowski F. Vancomycin-induced linear IgA disease with autoantibodies to BP 180 and LAD285. Br J Dermatol. 2001 Nov;145(5):816-20. PubMed
8. Zone JJ, Taylor TB, Meyer LJ, Petersen MJ. The 97 kDa linear IgA bullous disease antigen is identical to a portion of the extracellular domain of the 180 kDa bullous pemphigoid antigen, BPAg2. J Invest Dermatol. 1998 Mar;110(3):207-10. PubMed
9. Paul C, Wolkenstein P, Prost C, Caux F, Rostokor G, Heller M, Wechsler J, Revuz J, Roujeau JC. Drug-induced linear IgA disease: target antigens are heterogeneous. Br J Dermatol. 1997 Mar;136(3):406-11. PubMed
10. Nousari HC, Kimyai-Asadi A, Caeiro JP, Anhalt GJ. Clinical, demographic and immunohistologic features of vancomycin-induced linear IgA bullous disease of the skin. Report of 2 cases and review of the literature. Medicine (Baltimore). 1999 Jan;78(1):1-8. PubMed
11. Richards SS, Hall S, Yokel B, Whitmore SE. A bullous eruption in an elderly woman. Vancomycin-associated linear IgA dermatosis (LAD). Arch Dermatol. 1995 Dec;131(12):1447-8, 1450-1. No abstract available. PubMed
12. Whitworth JM, Thomas I, Peltz SA, Sullivan BC, Wolf AH, Cytryn AS. Vancomycin-induced linear IgA bullous dermatosis (LABD). J Am Acad Dermatol. 1996 May;34(5 Pt 2):890-1. PubMed
13. Neughebauer BI, Negron G, Pelton S, Plunkett RW, Beutner EH, Magnussen R. Bullous skin disease: an unusual allergic reaction to vancomycin. Am J Med Sci. 2002 May;323(5):273-8. PubMed
14. Wiadrowski TP, Reid CM. Drug-induced linear IgA bullous disease following antibiotics. Australas J Dermatol. 2001 Aug;42(3):196-9. PubMed
15. Kelly SE, Frith PA, Millard PR, Wojnarowska F, Black MM. A clinicopathological study of mucosal involvement in linear IgA disease. Br J Dermatol. 1988 Aug;119(2):161-70. PubMed
16. Kuechle MK, Stegemeir E, Maynard B, Gibson LE, Leifermen KM, Peters MS. Drug-induced linear IgA bullous dermatosis: report of six cases and review of the literature. J Am Acad Dermatol. 1994 Feb;30(2 Pt 1): 187-92. PubMed
17. Carpenter S, Berg D, Sidhu-Malik N, Hall RP 3rd, Rico MJ. Vancomycin-associated linear IgA dermatosis. A report of three cases. J Am Acad Dermatol. 1992 Jan;26(1):45-8. PubMed
18. Jablonska S, Chorzelski T. [IgA linear dermatosis (author's transl)]. Ann Dermatol Venereol. 1979 Sep;106(8-9):651-5. PubMed
19. Wojnarowska F, Marsden RA, Bhogal C, Black MM. Chronic bullous disease of childhood, childhood cicatricial pemphigoid, and linear IgA disease of adults: a comparative study demonstrating clinical and immunopathologic overlap. J Am Acad Dermatol. 1988 Nov;19(5 Pt 1):792-805. PubMed
20. Leonard JN, Haffenden GP, Ring NP, McMinn RM, Sidgwick A, Mowbray JF, Unsworth DJ, Holborrow EJ, Blenkinsopp WK, Swain AF, Fry L. Linear IgA disease in adults. Br J Dermatol. 1982 Sep;107(3):301-16 PubMed
21. Hughes AP, Callen JP. Drug-Induced Linear IgA bullous dermatosis mimicking toxic epidermal necrolysis. Dermatology. 2001;202(2):138-9. No abstract available. PubMed
© 2006 Dermatology Online Journal