Clear cell acanthoma induced by a dermatofibroma
Published Web Location
https://doi.org/10.5070/D358n6b3z3Main Content
Clear cell acanthoma induced by a dermatofibroma
David Silverstein1 MD, Ashfaq Marghoob2 MD
Dermatology Online Journal 18 (10): 14
1. SUNY Stony Brook, Stony Brook, New York2. Memorial Sloan Kettering
Abstract
Dermatofibromas are known to induce overlying skin changes and secondary lesions including seborrheic keratoses, Bowen disease, and basal cell hyperpigmentation. However, a paucity of literature describes clear cell acanthomas being induced by a dermatofibromas. We describe an unusual case of a clear cell acanthoma overlying a dermatofibroma and present the first dermoscopic image (to our knowledge) to the literature.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|
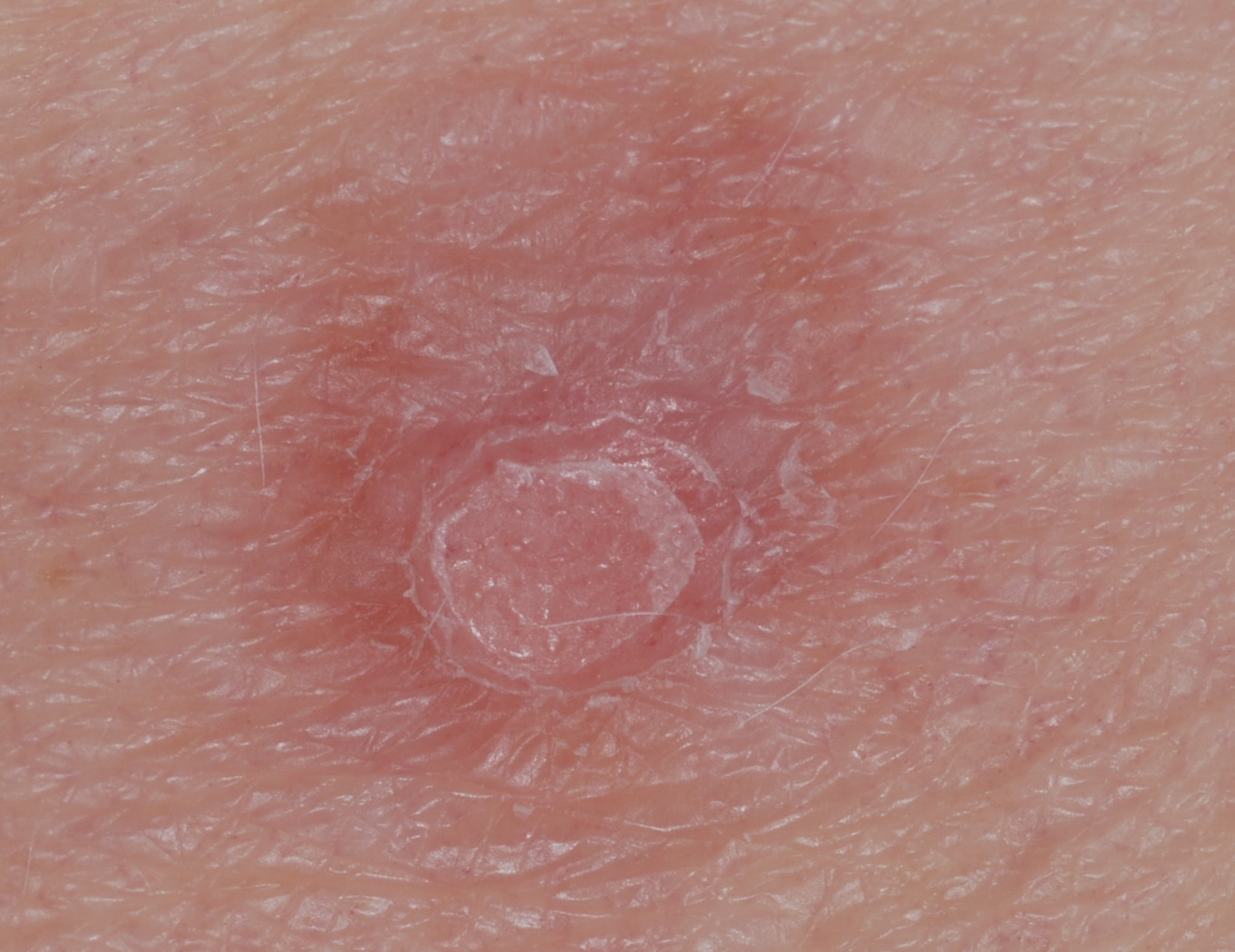
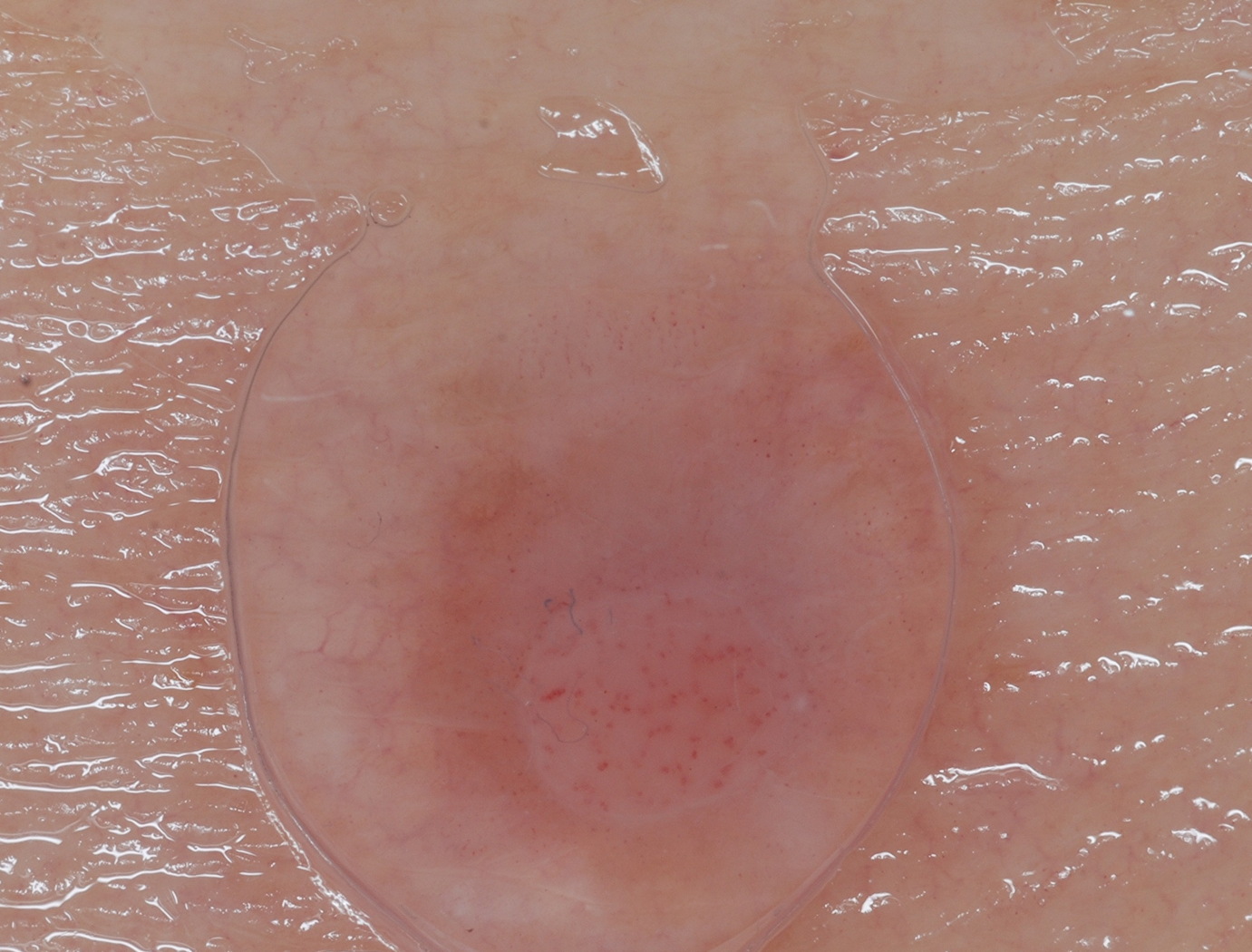
A 64-year-old woman with a history of multiple dysplastic nevi presented to our dermatology clinic for evaluation of a lesion on her left posterior arm. She was uncertain as to its duration and she denied any pain or bleeding from this lesion. She denied any associated systemic complaints. Physical examination revealed a 2 mm to 3 mm pink papule superimposed on a firm tan-colored 7 mm plaque (Figure 1). Dermoscopy of the lesion revealed a faint tan color and peripheral pigmented network surrounding a pale area, which contained dotted and glomerular vessels. These vessels were arranged in a serpiginous or string of pearls like configuration (Figure 2). A shave-excision of the lesion was performed (Figure 3).
Microscopic findings
 |
| Figure 3 |
|---|
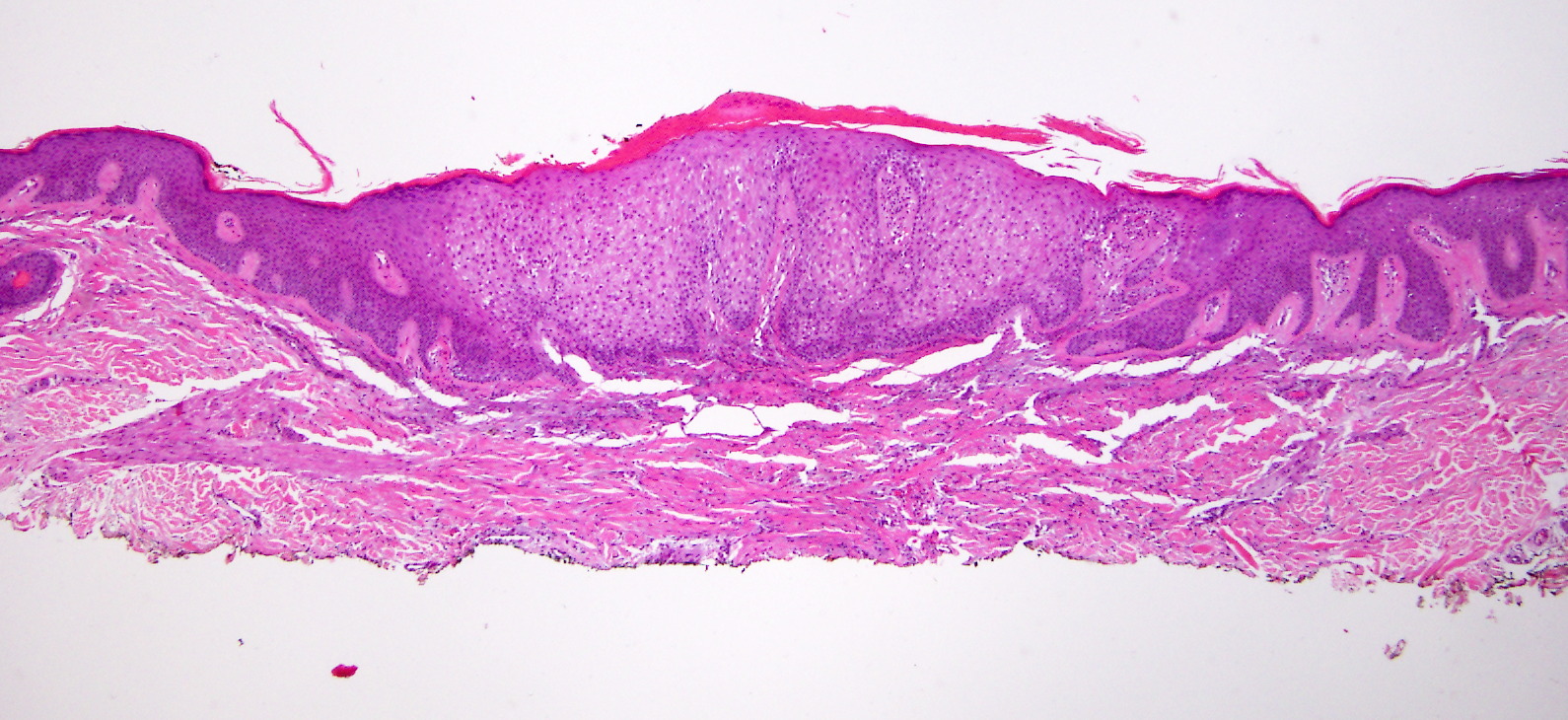
Histologic findings revealed a spindle-cell proliferation of cells in the dermis. The epidermis of the tan area revealed table-topping of the rete ridges in addition to basilar hyperpigmentation. Toward the center of the lesion a clear transition from normal-appearing keratinocytes to pale-staining keratinocytes with acanthosis was evident. These changes were consistent with a dermatofibroma with an overlying clear cell acanthoma.
Discussion
The dermoscopy of both dermatofibromas (DFs) and clear cell acanthomas (CCAs) is well-described [1, 2]. Clinically and dermoscopically, the architecture of this lesion was consistent with a DF because it was firm with a dimple sign and there was a peripheral faint network and tan pigment. The dermoscopy of the small papule was consistent with a CCA because it had a string of pearls distribution of dotted and glomerular vessels. This combined lesion is consistent with a DF with an overlying CCA as was supported histologically.
Alteration of the overlying epidermis by DFs is a well-described phenomenon in which acanthosis, pseuodoepitheliomatous hyperplasia, and basal layer hyperpigmentation have been described in addition to more unusual lesions including seborrheic keratoses, sebaceous hyperplasia, epidermolytic hyperkeratosis, focal acantholysis, Bowen disease, and follicular basal cell hyperplasia [3]. Indeed, some changes, especially the follicular basal cell hyperplasia, can be so pronounced as to cause histologic confusion in distinguishing basal cell carcinoma (BCC) from DF and this raises questions about the mechanism of the overlying skin changes and biologic behavior. In this regard, Morgan et al implicated overexpression of epidermal growth factor receptor (EGF-R) by the spindle cells in DFs as responsible for hyperplasia [4]. Additionally, Han et al found that the epidermal cells of DFs are relatively quiescent in their biologic activity, resembling terminally differentiated benign epidermis with respect to markers of differentiation when compared to cells of BCC [5]. Thus, the overlying epidermal changes have been referred to as induction and this likely represents a benign process of stimulated change in contrast to neoplastic transformation.
Whereas induction of the changes noted above is well described, there is a paucity of evidence in the literature regarding clear cell acanthoma-like changes. However, recently Shuweiter and Boer noted clear cell-like changes in 18.6 percent of DFs they studied, though they did not specify whether such changes corresponded clinically to the growth of distinct clear cell acanthoma-like papules [6]. Our case clearly shows a CCA and whereas this may be a chance collision of two benign lesions, it more likely represents a DF that has induced the formation of a CCA.
References
1. Zalaudek, I., et al., How to diagnose nonpigmented skin tumors: a review of vascular structures seen with dermoscopy: part II. Nonmelanocytic skin tumors. J Am Acad Dermatol, 2010. 63(3): p. 377-86; quiz 387-8. [PubMed]2. Zaballos, P., et al., Dermoscopy of dermatofibromas: a prospective morphological study of 412 cases. Arch Dermatol, 2008. 144(1): p. 75-83. [PubMed]
3. Cheng, L., S.B. Amini, and M. Tarif Zaim, Follicular basal cell hyperplasia overlying dermatofibroma. Am J Surg Pathol, 1997. 21(6): p. 711-8. [PubMed]
4. Morgan, M.B., H.G. Howard, and M.A. Everett, Epithelial induction in dermatofibroma: a role for the epidermal growth factor (EGF) receptor. Am J Dermatopathol, 1997. 19(1): p. 35-40. [PubMed]
5. Han, K.H., C.H. Huh, and K.H. Cho, Proliferation and differentiation of the keratinocytes in hyperplastic epidermis overlying dermatofibroma: immunohistochemical characterization. Am J Dermatopathol, 2001. 23(2): p. 90-8. [PubMed]
6. Shuweiter, M. and A. Boer, Spectrum of follicular and sebaceous differentiation induced by dermatofibroma. Am J Dermatopathol, 2009. 31(8): p. 778-85. [PubMed]
© 2012 Dermatology Online Journal