Segmental neurofibromatosis
Published Web Location
https://doi.org/10.5070/D34tp6q507Main Content
Segmental neurofibromatosis
Frank C Victor MD
Dermatology Online Journal 11 (4): 20
Department of Dermatology, New York University School of Medicine
Abstract
A 74-year-old man presented with skin-colored nodules in his left antecubital fossa. The lesions had been present for 35 years and were asymptomatic. Nodules elsewhere on the body, café-au-lait spots, axillary freckling, and Lisch nodules were absent. No family members had similar nodules. A diagnosis of segmental neurofibromatosis was made, and a biopsy specimen of a nodule showed a neurofibroma. As the patient had no complications of neurofibromatosis 1, no treatment was needed.
A 74-year-old man presented to the Veterans Affairs New York Harbor View Healthcare System dermatology service for evaluation of a red patch on his face; this was diagnosed as seborrheic dermatitis and was treated with Nizoral and hydrocortisone cream 2.5 percent. The patient also was noted to have lesions in the left antecubital fossa that had been present for more than 35 years. They had gradually increased in size over that time and were asymptomatic. He denied a history of other family members with similar lesions. Past medical history included an ulcer and benign prostatic hypertrophy. He denied history of cancer.
Eight, soft, skin-colored papules ranging in size from 3 to 7 mm were present in the left antecubital fossa. No similar lesions were found elsewhere. Axillary freckling, café-au-lait macules, plexiform neurofibromas, and Lisch nodules were not present.

|
|
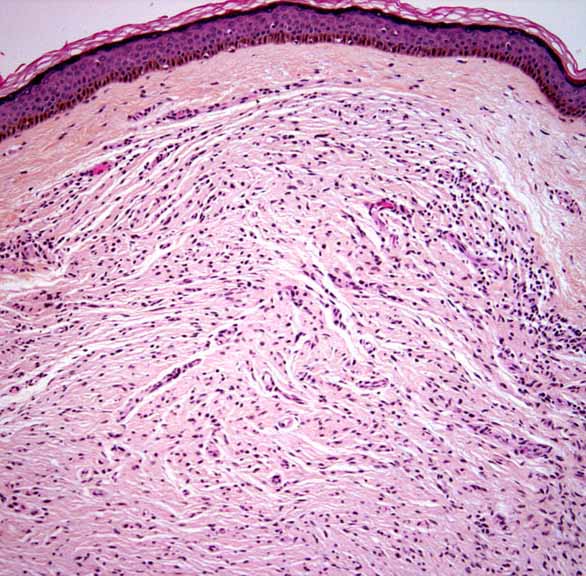
| Figure 1 | Figure 2 |
|---|
Histopathology reveals a well-circumscribed spindle-cell neoplasm whose cells are arranged as fascicles and have oval or spindle-shaped, wavy nuclei and scant cytoplasm. Nuclear pleomorphism and mitoses are not evident.
Comment
Segmental neurofibromatosis (NF) is a rare disorder that is characterized by neurofibromas, with or without pigmentary changes, that are localized most often to one region of the body. Its prevalence is estimated between 0.0014 and 0.002 percent [1]. Segmental NF is an example of mosaicism, in which localized disease results from a postzygotic NF1 gene mutation. Gene mutations can arise in both somatic and gonadal cell lines. Gonadal mosaicism is thought to be responsible for reports of patients with localized disease having children with generalized NF [1, 2]. Vertical transmission of segmental NF has also been reported although the mode of inheritance is unclear and not easily explained by gonadal mosaicism [1].
Segmental NF initially was classified as NF type V and defined as café-au-lait macules or neurofibromas in a single, unilateral segment of the body, with no crossing of the midline, no familial history, and no systemic involvement [3]. Cases that did not conform to these criteria prompted further classification into the following subtypes: true segmental, localized with deep involvement, hereditary, and bilateral [3].
Clinically, patients may be divided into four groups: those with only pigmentary changes or neurofibromas, those with both pigmentary changes and neurofibromas, and those with isolated plexiform neurofibromas. Lesions are usually unilateral although there are reports of bilateral segmental NF [4, 5]. Clinical disease develops along the same time course as generalized NF with pigmentary changes and plexiform neurofibromas developing in childhood and neurofibromas in adulthood [1]. Most commonly, patients present with only neurofibromas. The neurofibromas are most always asymptomatic and range in size from 0.1 cm to several centimeters in diameter. They tend to arise in a dermatomal distribution, most commonly cervical, followed by thoracic, lumbar, and sacral [6]. Pigmentary changes include café-au-lait macules and axillary freckling, with the former being more common [6]. In most cases, pigmentary changes seem to follow the lines of Blaschko [1]. Isolated plexiform neurofibromas are rare and most of those reported are localized to the head or neck [1]. Some patients with segmental NF have had complications of NF1, which have included learning difficulties, optic pathway gliomas, and pseudoarthrosis. Those with learning difficulties tended to have more extensive areas of cutaneous involvement [1]. Lisch nodules are rarely seen in segmental NF.
There are no specific guidelines regarding management for segmental NF. Patients should be informed that they do not have generalized NF1 and that their risk of disease-associated complications is low [1].
References
1. Ruggieri M, et al. The clinical and diagnostic implications of mosaicism in the neurofibromatoses. Neurology 2000; 56:14332. Oguzkan S, et al. Familial segmental neurofibromatosis. J Child Neurol 2004;19:392
3. Ingordo CDR, et al. Segmental neurofibromatosis: is it uncommon or underdiagnosed? Arch Dermatol 1995;131: 959
4. Cecchi R, et al. Bilateral segmental neurofibromatosis. Dermatology 1992;185:59
5. Nagaoka Y, et al. Bilateral segmental neurofibromatosis. Acta DermVenereol (Stockh) 2002;82:219
6. Hager CM, et al. Segmental neurofibromatosis: case reports and review. J Am Acad Dermatol 1997;37: 864
© 2005 Dermatology Online Journal