Multiple lentigines confined to a resolving psoriatic plaque
Published Web Location
https://doi.org/10.5070/D34df1z0p5Main Content
Multiple lentigines confined to a resolving psoriatic plaque
Nuria Martí MD1, Inmaculada Molina MD1, Verónica López MD1, Liria Terradez MD2, Esperanza Jordá MD, PhD1
Dermatology Online Journal 15 (10): 15
1. Department of Dermatology, Hospital Clínico Universitario, Valencia, Spain. nuriamarfa@hotmail.com2. Department of Pathology, Hospital Clínico Universitario, Valencia, Spain
Abstract
Development of nevus spilus-like lentigines in zones previously affected by plaques of psoriasis has been described. Most cases have appeared following phototherapy; then it has been suggested that the mechanism involved could be an abnormal reaction to UV light. However, cases of multiple lentigines arising within resolving psoriatic in patients who had not received phototherapy or photochemotherapy have been described as a result of possible post-inflammatory hyperpigmentation. We report the case of patient who developed nevus spilus-like lentigines following therapy with topical calcipotriol on psoriatic plaques. We consider that the mechanism of production of lentigines is an unusual form of postinflammatory hyperpigmentation.
Development of nevus spilus-like lentigines in zones previously affected by plaques of psoriasis has been described [1]. Most cases have appeared following phototherapy; then it has been suggested that the mechanism involved could be an abnormal reaction to UV light [1, 2]. However, cases of multiple lentigines arising within resolving psoriatic plaques in patients who had not received phototherapy or photochemotherapy have been described as a result of possible post-inflammatory hyperpigmentation [1, 3, 4]. We report the case of patient who developed nevus spilus-like lentigines following therapy with topical calcipotriol on psoriatic plaques. We consider that the mechanism of production of lentigines is an unusual form of postinflammatory hyperpigmentation.
 |  |
| Figure 1A | Figure 1B |
|---|---|
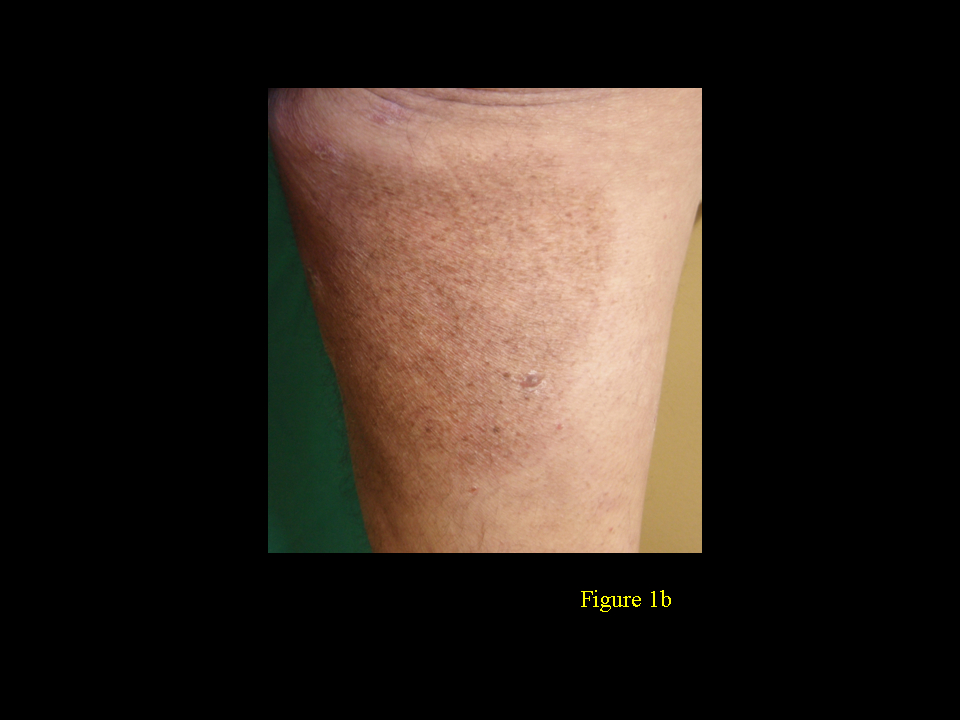
| Figure 1. Hyperpigmentation in the trunk (A) and in the thigh (B) | |
The patient was a 65-year-old man (Fitzpatrick phototype 2) who presented with psoriasis plaques of 30 years duration. His psoriasis had been treated only with topical corticosteroids and he had not received phototherapy or any other immunosuppressive treatment. We changed his topical treatment to calcipotriol ointment. Three months after the beginning of calcipotriol therapy, we observed the appearance of small dark brown macules within light brown macules on his trunk, buttocks and extremities (Figs. 1A & 1B). These nevus spilus-like lentigines appeared at the site of resolution of the thick plaque of psoriasis. No phototherapy was used and there had been no sunexposure of the affected area during the period of treatment. No pigmentary sequelae developed at the site of other less thick psoriatic lesions treated with calcipotriol alone.
 |  |
| Figure 2A | Figure 2B |
|---|---|
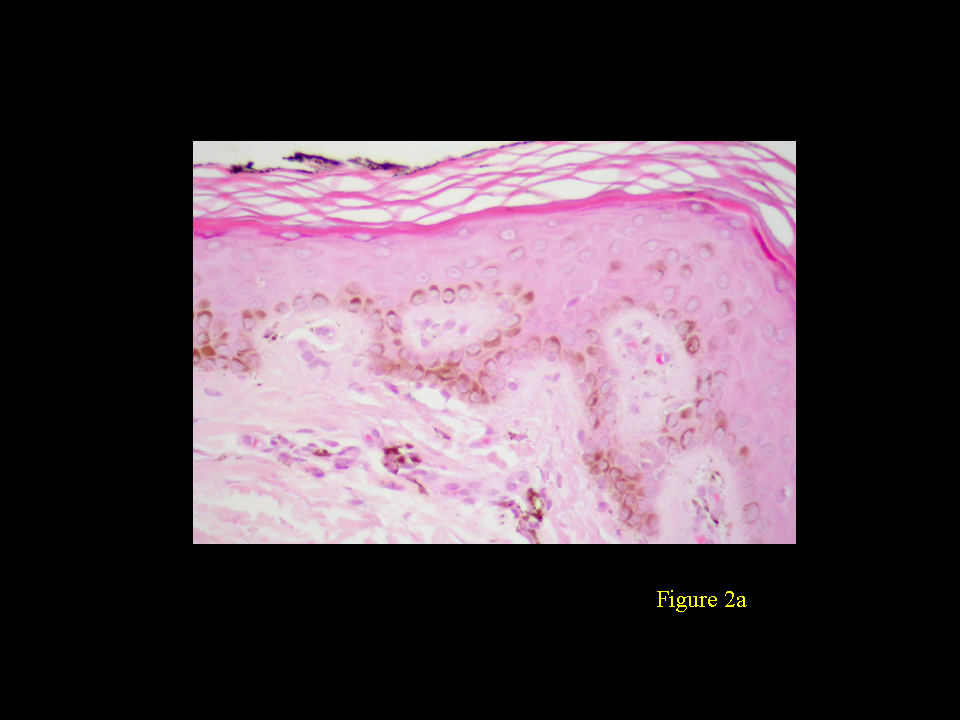
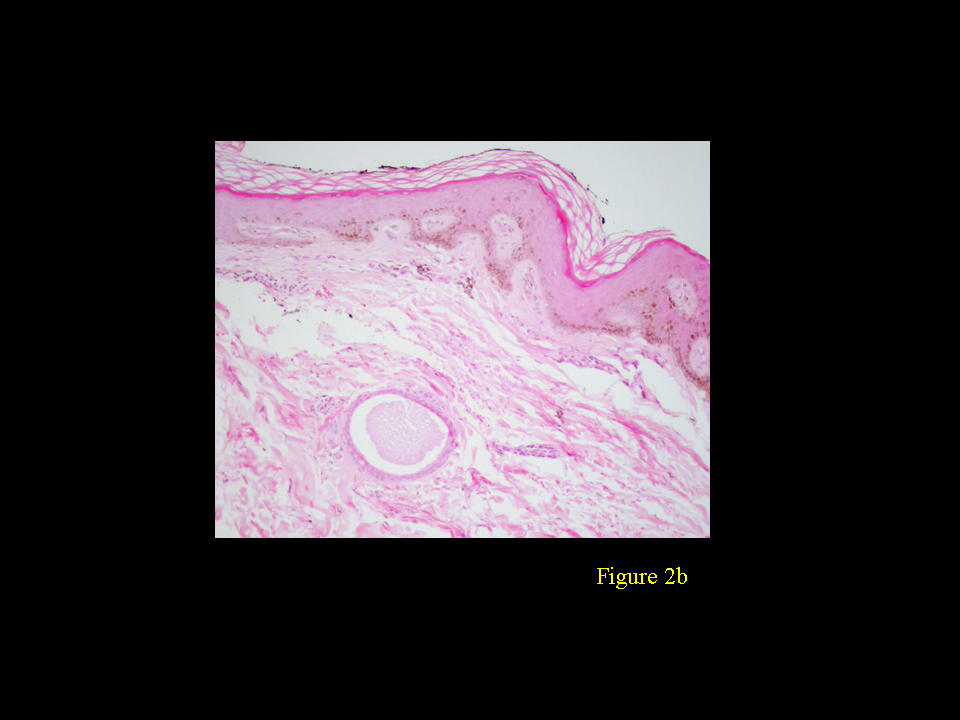
| Figure 2A. Hyperpigmentation of the basal layer with melanophages in the upper dermis (H&E, x150) Figure 2B. Basal cell hyperpigmentation and elongation of the rete ridges with some anastomoses between them (H&E, x300) | |
Histopathological examination revealed basal cell hyperpigmentation and elongation of the rete ridges with some anastomoses between them. There were melanophages in the upper dermis (Figs. 2A & 2B). Although the patient had been treated several times before by topical corticosteroids without any signs of lesional hyperpigmentation, the occurrence only in the more severe plaque points to some unusual form of post-inflammatory hyperpigmentation. Calcipotriol is known to cause a local irritative reaction in the skin, which could lead to the development of post-inflammatory pigmentation. Some authors have reported that 1,25-dihydroxyvitamin D3 is involved in the regulation of melanin synthesis and melanocytes have been shown to express 1,25-dihydroxyvitamin D3 receptors, but their exact role in melanogenesis is not yet clear [1, 5]. On the other hand, post-inflammatory hypomelanotic areas occuring following the resolution of psoriasis is well documented and topical corticosteroids have also been reported to cause melanocytic inhibition [6]. Recently, development of lentigines after using biologic drugs has been described [7, 8]. We consider that the mechanism of production of lentigines is related to inflammation and not to the therapy used.
References
1. Burrows NP, Handfield-Jones S, Monk BE, et al. Multiple lentigines confined to psoriatic plaques. Clin Exp Dermatol 1994; 19:380-2. [PubMed]2. Basarab T, Millard TP, McGregor JM, Barker JN. Atypical pigmented lesions following extensive PUVA therapy. Clin Exp Dermatol 2000; 25:135-7. [PubMed]
3. Dawn G, McHenry P, Burden AD. Lentigines in psoriatic plaques: are they unique? Clin Exp Dermatol. 2001; 26(5):459. [PubMed]
4. Rogers M. Multiple lentigines confined to a resolving psoriatic plaque, treated without phototherapy. Clin Exp Dermatol. 1995; 20(5):446. [PubMed]
5. Gläser R, Röwert J, Mrowietz U. Hyperpigmentation due to topical calcipotriol and photochemotherapy in two psoriatic patients. Br J Dermatol. 1998; 139(1):148-51. [PubMed]
6. Mahendran R, Norris PG. Multiple lentigines clearing in resolving psoriatic plaques. Clin Exp Dermatol. 1999; 24(3):237. [PubMed]
7. Costa LA, Belinchón I, Betlloch I, Pérez-Crespo M, Mataix J. Multiple lentigines arising in resolving psoriatic plaques alter treatment wiht etarnecept. Dermatol Online J. 2008 Jan 15;14(1):11. [PubMed]
8. Santos-Juanes J, Coto P, Mallo S et al. Multiple lentigines confined to resolving psoriatic plaques in a patient treated with adalimumab. Dermatology. 2008; 216(3):279. [PubMed]
© 2009 Dermatology Online Journal