Necrobiotic xanthogranuloma
Published Web Location
https://doi.org/10.5070/D34566x4hjMain Content
Necrobiotic xanthogranuloma
Sue Ann Wee MD and Jerome L Shupack MD
Dermatology Online Journal 11 (4): 24
Department of Dermatology, New York University School of Medicine
Abstract
A 67-year-old man presented with a 13-year history of slowly enlarging yellow-red plaques on the face and lower extremity. A biopsy specimen was consistent with necrobiotic xanthogranuloma. Necrobiotic xanthogranuloma is a slowly progressive histiocytic disease that is associated with paraproteinemia in most cases; however, its pathogenesis remains unclear. Although there is no first-line therapy, anecdotal reports have shown variable benefit with chemotherapeutic agents.
About 13 years ago, a 67-year-old man developed a papule on his left temple with the subsequent appearance of multiple papules on the remainder of his face and proximal extremities. Over the years, the papules gradually coalesced into plaques over his face, with sparing of the upper and lower eyelids and perioral region. There was persistence of skin lesions despite therapy with topical glucocorticoids, Nd-YAG laser, and local surgical excision. Past medical history includes idiopathic thrombocytopenia that was treated with splenectomy.

|

|
| Figure 1 | Figure 2 |
|---|
|
| Figure 3 |
|---|
Hematocrit was 52.2 percent and platelet count 33 x 109/L. Protein electrophoresis showed a spike in the gamma region, which reflected an elevated gamma-globulin level of 1.6 gm/dL. There were also elevated IgG (heavy chain) and IgE levels of 1820 mg/dL and 364 IU/ml, respectively. The erythrocyte sedimentation rate was 14 mm/hr.
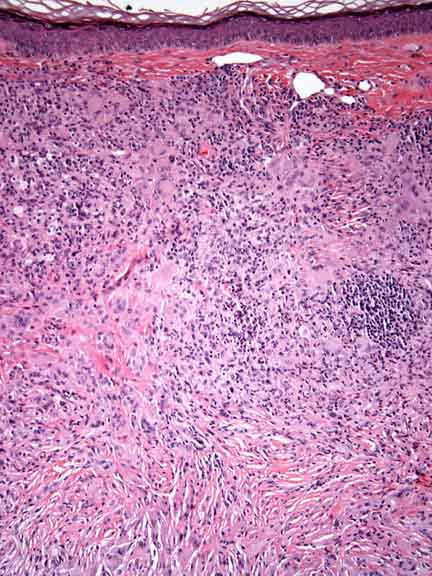
Histopathology reveals a diffuse, predominantly granulomatous infiltrate of foamy and multinucleated histiocytes, many of which are of the Touton type. There are also numerous neutrophils with focal abscess formation. Necrobiosis and cholesterol clefts are not evident.
Comment
Necrobiotic xanthogranuloma (NXG) is a rare, progressive, histiocytic disease that features destructive cutaneous lesions, a close association with paraproteinemia, and multisystem extracutaneous manifestations. NXG is a disease of adults with an average age of onset in the sixth decade [1, 2]. NXG begins as papules and nodules that slowly enlarge into indurated plaques. Characteristic lesions have a red-orange or yellow color as well as telangiectases, atrophy, scars, and ulcers [1, 2]. The most common site of involvement is the face, particularly the periorbital region (85 % of cases); the trunk and proximal extremities are other affected sites [2]. Ophthalmologic complications affect approximately 50 percent of cases and include orbital masses, conjunctival involvement, keratitis, scleritis, and uveitis [1, 2].
NXG may involve other extracutaneous sites, including the heart, lungs, kidneys, liver, spleen, intestines, skeletal muscle, and central nervous system [3, 4]. Paraproteinemia is closely associated with NXG, with approximately 80 percent of patients demonstrating a monoclonal gammopathy on serum protein electrophoresis; furthermore, 10 percent of these patients develop multiple myeloma [2]. Other lymphoproliferative disorders such as Hodgkin's lymphoma have been associated with NXG [5]. Hepatosplenomegaly, an increased erythrocyte sedimentation rate, leukopenia, hypocomplementemia, and cryoglobulinemia are other common findings [1, 2].
The link between paraproteinemia and NXG remains unclear. Theories regarding pathogenesis include deposition of immunoglobulins and lipid complexes with a foreign body giant-cell reaction and monocyte activation with intracellular lipid accumulation [6]. Histopathologic examination shows a palisading xanthogranuloma with areas of necrobiotic, degenerated collagen that infiltrates the mid-dermis with extension into the subcutaneous fat. Multiple xanthomatized histiocytes, touton giant cells, other bizarre giant cells, cholesterol clefts, and lymphoid follicles are often present within granulomas [1].
Only anecdotal reports are available to support treatment options for NXG. Improvement in skin lesions has been seen with chlorambucil, melphalan, localized radiotherapy, systemic glucocorticoids, interferon α-2a, and plasmapheresis with hydroxychloroquine [7, 8, 9, 10, 11, 12].
References
1. Finan MC, Winkelmann RK. Necrobiotic xanthogranuloma with paraproteinemia: a review of 22 cases. Medicine 1986;65:3762. Mehregan DA, Winkelmann RK. Necrobiotic xanthogranuloma. Arch Dermatol 1992;128:94
3. Winkelmann RK, et al. Giant cell granulomatous pulmonary and myocardial lesions in nerobiotic xanthogranuloma with paraproteinemia. Mayo Clin Proc 1997;72:1028
4. Shah KC, et al. Necrobiotic xanthogranuloma with cutaneous and cerebral manifestations. J. Neurosurg 2004;100:1111
5. Reeder CB, et al. The evolution of Hodgkin's disease and necrobiotic xanthogranuloma syndrome. Mayo Clin Proc 1991;66:1222
6. Matsura F, et al. Activation of monocytes in vivo causes intracellular accumulation of lipoprotein-derived lipids and marked hypocholesterolaemia: a possible pathogenesis of necrobiotic xanthogranuloma. Atherosclerosis 1999;142:355
7. Machado S, et al. Cutaneous necrobiotic xanthogranuloma - successfully treated with low dose chlorambucil. Eur J Dermatol 2001;11:458
8. Macfarlane AW, Verbov JL. Necrobiotic xanthogranuloma with paraproteinaemia. Br J Dermatol 1985;113:339
9. Char DH, et al. Radiation therapy for ocular necrobiotic xanthogranuloma. Arch Ophthalmol 1987;105:174
10. Chave TA, et al. Recalcitrant necrobiotic xanthogranuloma responding to pulsed high-dose oral dexamethasone plus maintenance therapy with oral prednisolone. Br J Dermatol 2001;144:158
11. Georgiou S, et al. Interferon alpha-2a monotherapy for necrobiotic xanthogranuloma. Acta Derm Venereol (Stockh) 1999;79:484
12. Finelli LG, Ratz JL. Plasmapheresis, a treatment modality for necrobiotic xanthogranuloma. J Am Acad Dermatol 1987;17:351
© 2005 Dermatology Online Journal