Generalized granuloma annulare
Published Web Location
https://doi.org/10.5070/D341x2d4r2Main Content
Generalized granuloma annulare
Olympia Kovich MD and Susan Burgin MD
Dermatology Online Journal 11 (4): 23
Department of Dermatology, New York University School of Medicine
Abstract
A 94-year-old man presented with a relatively asymptomatic eruption of his forearms, abdomen, and back comprising symmetric erythematous papules and plaques. Generalized granuloma annulare is an idiopathic disorder that occurs more commonly in older patients and is characterized by numerous flesh-colored-to-erythematous papules. It is distinguished histologically by palisading granulomas with central connective tissue degeneration and with central mucin. Therapy has been attempted with various modalities with moderate efficacy.
A 94-year-old man with a history of chronic lymphocytic leukemia presented with a 1-year history of a pruritic eruption that initially began on his wrists and forearms. It subsequently spread to his central abdomen and back. The patient attributed the onset of the eruption to a change in medication from rabeprazole to omeprazole. He reported that the lesions were fading after discontinuing omeprazole. A biopsy was performed to confirm the diagnosis. Treatment was initiated with fluocinonide ointment, with moderate improvement. A 3-month trial of doxycyline 100 mg twice daily was subsequently discontinued because of gastrointestinal side effects. The patient did report improvement of the eruption with this therapy. After discontinuation of doxycycline, the patient felt that sufficient resolution had been achieved and opted to continue only topical therapy with fluocinonide ointment. The eruption did not flare with re-initiation of rabeprazole therapy.
Physical examination revealed erythematous-violaceous annular plaques with raised borders on the wrists. Flat-topped, erythematous papules were present on the abdomen and back.

|
|
| Figure 1 | Figure 2 |
|---|
The lipid profile and a glucose level were normal
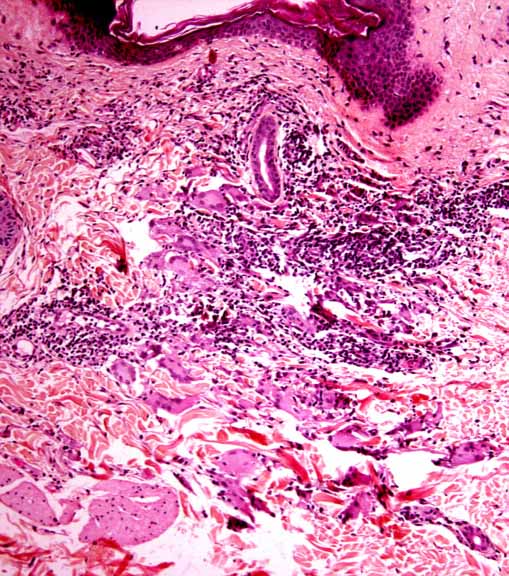
Histopathology reveals a palisaded granulomatous infiltrate of lymphocytes and histiocytes around a central zone of degenerated collagen; many of the histiocytes are multinucleated and exhibit elastophagocytosis.
Comment
Granuloma annulare is a common, idiopathic disorder, which occurs twice as commonly in women. The age of onset is usually prior to age 30. Although no clear etiology has been established, insights into the pathogenesis include the observation of a Th-1 cytokine profile expressed by T cells in lesions [1]. The true inciting agent that elicits a delayed-type hypersensitivity reaction is unknown, but various associations have been reported; these include diabetes mellitus, malignant conditions, thyroid disease, acquired immunodeficiency syndrome, hepatitis C, and other viral infections [2]. Familial cases of granuloma annulare are also reported [1].
Clinical variants of granuloma annulare include localized, generalized, subcutaneous, micropapular, nodular, perforating, and (rarely) pustular generalized perforating granuloma annulare [1, 3]. Approximately 15 percent of patients have more than ten lesions and are thus considered to have generalized granuloma annulare. This subset of patients has typically a later onset of disease, lack of response to therapies, and an increased prevalence of the HLA-Bw35 allele [1]. Lesions have a predilection for the forearms, proximal aspects of the extremities, and trunk. They may present as skin-colored papules, small annular plaques, or large violaceous patches with elevated borders [4]. Alterations in the lipid profile (hypercholesterolemia, hypertriglyceridemia, or both) were found to occur in 45 percent of patients with generalized granuloma annulare [1]. Generalized granuloma annulare may represent a paraneoplastic phenomenon in patients with lymphoma or other malignant conditions [1, 5].
Lesions of granuloma annulare are distinguished histologically by palisading granulomas with central connective tissue degeneration and with central mucin [1]. Although elastophagocytosis may be observed, it is a more prominent finding in annular elastolytic giant-cell granuloma [1]. Evidence of vascular involvement on histopathologic examination may indicate an underlying systemic disease [1]. Although no laboratory tests are diagnostic, a serum blood glucose, complete blood count with differential analysis, lipid profile, and hepatitis-C antibody screening may be indicated.
Treatment has been attempted with topical and oral glucocorticoids, hydroxychloroquine, dapsone, cryosurgery, niacinamide, cyclosporine, chlorambucil, retinoids and PUVA photochemotherapy [1, 6]. A small case series reported resolution of generalized granuloma annulare with vitamin E and zileuton [4]. Regression with α-interferon in a patient with concomitant hepatitis C has been reported [2]. Doxycyline has not been reported in the treatment of granuloma annulare, but tetracyclines have reported efficacy in the treatment of sarcoidosis [7].
References
1. Howard A, White Jr CR. Non-infectious granulomas. In: Bolognia JL, et al., eds. Dermatology. Mosby: London, 2003:14552. Granel B, et al. Chronic hepatitis C virus infection associated with a generalized granuloma annulare. J Am Acad Dermatol 2000;43:918
3. Villegas RG, et al. Pustular generalized perforating granuloma annulare. Br J Dermatol 2003;149:866
4. Smith KJ, et al. Treatment of disseminated granuloma annulare with a 5-lipoxygenase inhibitor and vitamin E. Br J Dermatol 2002;146:667
5. Bhushan M, et al. Lymphoepithelioid lymphoma (Lennert's lymphoma) presenting as atypical granuloma annulare. Br J Dermatol 2000;142:776
6. Morita K, et al. Papular elastolytic giant cell granuloma: a clinical variant of annular elastolytic giant cell granuloma or generalized granuloma annulare? Eur J Dermatol 1999;9:647
7. Bachelez H, et al. The use of tetracyclines for the treatment of sarcoidosis. Arch Dermatol 2001;137:69
© 2005 Dermatology Online Journal