Extragenital lichen sclerosus et atrophicus
Published Web Location
https://doi.org/10.5070/D33g0275rmMain Content
Extragenital lichen sclerosus et atrophicus
Kendra G Bergstrom MD, Stephanie J Mengden MD, Hideko Kamino MD, David Ramsay MD
Dermatology Online Journal 14 (5): 23
Department of Dermatology, New York UniversityAbstract
A 76-year-old woman with a history of eczematous dermatitis presented with a 9-month history of a pruritic, eczematous eruption of the trunk. This eruption responded to topical glucocorticoids but recurred multiple times after discontinuation of treatment. A biopsy specimen showed extragenital lichen sclerosus et atrophicus. The diagnosis of extragenital lichen sclerosus is reviewed with a comparison to classic lichen sclerosus in terms of clinical features, histopathologic characteristics, and treatment approaches.
Clinical synopsis
A 76-year-old woman with a history of a pruritic, scaly eruption on the back, abdomen, and inguinal folds for 9 months was referred to the Charles C. Harris Skin and Cancer Pavilion for further evaluation. The eruption initially was noted during a hospitalization. Initial treatment with topical glucocorticoids improved the itching without resolution of the eruption. An initial biopsy was taken. On further evaluation, 2 other biopsies were taken. Review of systems was negative for fever, chills, weight loss, or fatigue. Past medical history included colon cancer status-post resection, coronary-artery disease, arthritis, emphysema, and cataracts.
Physical Examination
Hyperpigmented, atrophic, 1-cm to 6-cm, thin plaques were present on the flanks, shoulders, and inframammary area. Vaginal skin was without lesions. Lymphadenopathy and hepatosplenomegaly were absent.
 |  |
| Figure 1 | Figure 2 |
|---|
A complete blood count, comprehensive metabolic panel, and thyroid function were normal. Antinuclear antibody was negative and rapid plasma reagin test was non-reactive. Serum protein electrophoresis and immunofixation showed no monoclonal increase in immunoglobulins.
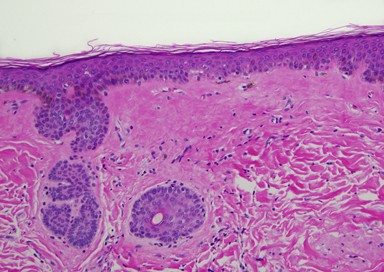
Histopathology
There is a sparse, superficial, perivascular, lymphohistiocytic infiltrate and sclerosis of the papillary dermis. The overlying atrophic epidermis demonstrates mild basal vacuolar change and slight, compact orthokeratosis.
Comment
The first report of lichen sclerosus et atrophicus (LS) was by Francois Henri Hallopeau in 1887, who described an atrophic form of lichen planus [1]. LS is an acquired, chronic, inflammatory skin disease that encompasses balanitis xerotica obliterans of the penis, kraurosis vulvae, and lichen sclerosus elsewhere on the body. Its prevalence is estimated at up to 0.3 percent [2]. Women are affected 10 times as often as are men, which is a statistic that may be influenced by early male circumcision.
The association of specific HLA types and other autoimmune diseases suggests that LS is an autoimmune process [3]. Other autoimmune diseases are observed in up to 33% of women, particularly thyroid disease, alopecia areata, and pernicious anemia [4]. IgG antibodies targeting extracellular matrix protein-1 (ECM1) are present in up to 75 percent of patients [5]. These antibodies are IgG2 and attach to different parts of the ECM1 molecule. No association has been observed between antibody titer, type, and clinical response [6]. The exact role of this antibody in disease pathogenesis has yet to be elucidated.
Initial lesions of LS are porcelain white papules, plaques, or atrophic patches that may be surrounded by an erythematous or violaceous halo. Itching may be severe, particularly in the genital form. Early lesions may show folliculocentric keratin plugs overlying follicular ostia. Bullae may appear with or without underlying hemorrhage. A Koebner reaction is common. Late lesions show atrophy, loss of pigmentation, and loss of normal skin markings. Other processes may be concurrently present, specifically morphea, lichen planus, or atrophoderma of Pasini and Pierini.
Extragenital LS is most often found on the chest, upper back, and breasts. Cases of linear LS have been reported along the lines of Blashko [7]. Clinically, hypopigmented atrophic patches are observed, which may or may not be pruritic. Histopathlogically, these lesions were likely to show concominant changes of lichen simplex chronicus or dermal eosinophils in one series [8]. Extragenital LS showed decreased expression of the proliferation marker Ki-67 and p53 in comparison to genital LS, which may explain in part the lack of reported malignant transformation in the extragenital subtype [9].
Although no reports exist of carcinoma arising in extragenital LS, LS is associated with increased risk of squamous-cell carcinoma (SCC) in genital skin. This risk approaches 5 percent in women and can be reduced with treatment of the underlying process [10]. Unlike other genital SCC, human papilloma virus (HPV) is only found in about 15 percent of cases [11]. The risk of penile SCC is lower in men. However, carcinomas may harbor HPV in up to 55 percent of cases.
Successful treatment of extragenital LS has been reported with ultraviolet B phototherapy and calcipotriene [12, 13]. The first-line treatment for all types of LS is the use of superpotent topical glucocorticoids. For patients unable to tolerate glucocorticoids or who do not have a satisfactory response, tacrolimus ointment also has demonstrated efficacy. Clinical trial data exists for the use of topical and oral retinoids for treatment of recalcitrant disease and case reports demonstrate efficacy for PUVA photochemotherapy, UVA1 phototherapy, and antimalarials. Topical testosterone has not shown benefit.
References
1. Hallopeau H. Lichen plan sclereux. Ann Dermatol Syphilol 1889; 10:4472. Tasker GL, et al. Lichen sclerosus. Clin Exp Dermatol 2003; 28: 128
3. Gao XH, et al. The association between HLA DR, DQ antigens, and vulval lichen sclerosus in the UK. J Invest Dermatol 2005;125:895
4. Harrington CI, et al. An investigation into the incidence of auto-immune disorders in patients with lichen sclerosus and atrophicus. Br J Dermatol 1981; 104: 563
5. Oyama N, et al. Autoantibodies to extracellular matrix protein 1 in lichen sclerosus. 2003; 362: 118
6. Chan I, et al. Characterization of IgG autoantibodies to extracellular matrix protein 1 in lichen sclerosus. Clin Exp Dermatol 2004; 29: 499
7. Choi SW, et al. A case of extragenital lichen sclerosus following Blaschko's lines. J Am Acad Dermatol 2000; 43:903
8. Carlson JA, et al. Clinicopathologic comparison of vulvar and extragenital lichen sclerosus: histologic variants, evolving lesions, and etiology of 141 cases. Mod Pathol 1998;11:844
9. Scurry J, et al. Histology of lichen sclerosus varies according to site and proximity to carcinoma. Am J Dermatopathol 2001; 23:413
10. Renaud-Vilmer C, et al. Vulvar lichen sclerosus: effect of long-term topical application of a potent steroid on the course of the disease. Arch Dermatol 2004;140:709
11. Ansink AC, et al. Human papilloma virus, lichen sclerosus and squamous cell carcinoma of the vulva: detection and prognostic significance. Gynaecol Oncol 1994; 52:180
12. Colbert RL, et al. Progressive extragenital lichen sclerosus successfully treated with narrowband UV-B phototherapy. Arch Dermatol 2007;143:19
13. Kreuter A, et al. Extragenital lichen sclerosus successfully treated with topical calcipotriol: evaluation by in vivo confocal laser scanning microscopy. Br J Dermatol 2002;146:332
© 2008 Dermatology Online Journal