Bilateral retro-auricular milia en plaque: A case report and review of the literature
Published Web Location
https://doi.org/10.5070/D339k433vgMain Content
Bilateral retro-auricular milia en plaque: A case report and review of the literature
Zahra Hallaji MD, Maryam Akhyani, Samaneh Jamshidi, Amirhossein Modabbernia MD, Kambiz Kamyab
Dermatology Online Journal 16 (1): 12
Department of Dermatology, Razi skin hospital, Faculty of Medicine, Tehran University of medical sciences, Tehran, Iran. Zhallaji@yahoo.comAbstract
Milia en plaque, a rare inflammatory plaque type of milia is generally located in the periauricular area. Bilateral retroauricular milia en plaque is very rarely reported. Here, we report another case of bilateral retroauricular milia en plaque and review the previous cases.
Introduction
Milia en plaque (MEP) is a rare inflammatory variant of milia that occurs on an erythematous base and is commonly found near the ear. Its etiology remains unrecognized in most cases. Bilateral retroauricular milia en plaque has been rarely reported.
Case report
Our patient was a 35-year-old female who presented with a one-year history of bilateral itchy lesions behind the ear. She had self-treated with clobetasol propionate, which was not helpful. There was no history of medical problems in the patient and she reported no trauma (wearing eyeglasses, abrasion, radiation); she applied no external agents such as cosmetics or perfumes. Also there was no history of corticosteroid use prior to the onset of the condition. There was no family history for any similar lesions or the presence of hereditary or rheumatologic disorders.
 |  |
| Figure 1a | Figure 1b |
|---|---|
| Figures 1a and 1b. Multiple tiny cysts (milia) upon an erythematous base in both retroauricular areas | |
Upon physical examination of the skin of the retroauricular area there were well defined erythematous plaques studded with multiple milia behind both ears (Figure 1). No other skin, nail, hair, or mucous membrane abnormalities were recognized.
 |  |
| Figure 2 | Figure 3 |
|---|---|
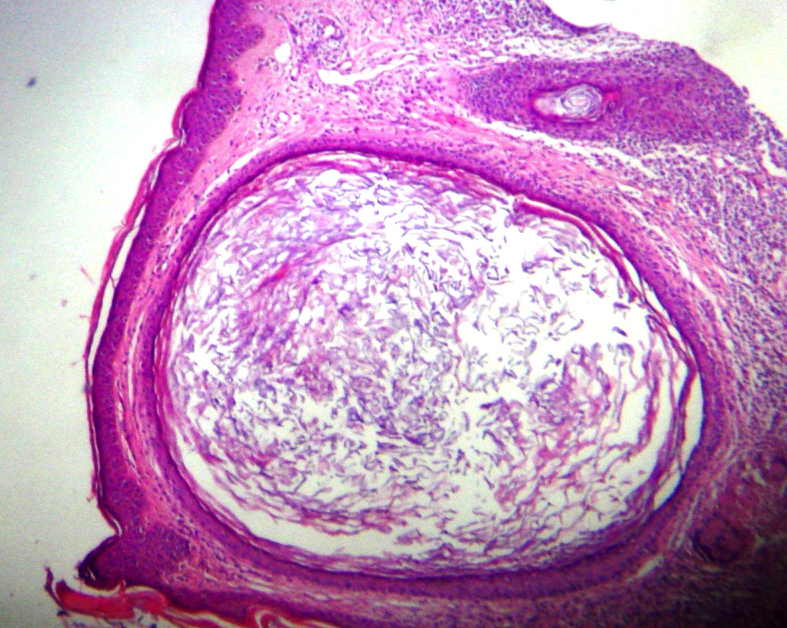
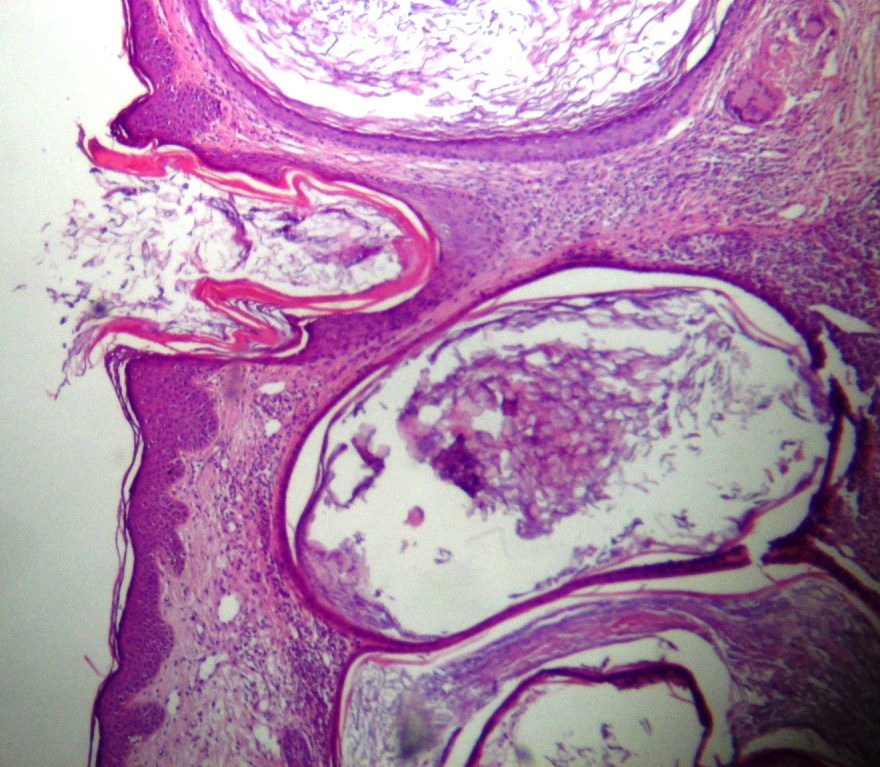
| Figures 2 and 3: Moderate lymphocytic infiltration (H&E, x100) | |
The biopsy of the lesion showed small keratin-filled cysts, which were enveloped by an epithelium of stratified squamous type. A moderate lymphocytic infiltration was present around the cysts (Figures 2 and 3).
Laboratory examination showed no abnormality in routine tests including blood count, ESR, kidney function tests and collagen vascular screening tests (ANA, C3, C4 and CH50).
Milia were evacuated and our patient was advised to avoid local irritants as well as administration of corticosteroids.
Discussion
Milia en plaque is a rare skin problem characterized by multiple keratin cysts (milia) located on an erythematous plaque; it commonly occurs in the retroauricular area [1]. In addition, others sites described include pre-auricular, supraclavicular, periorbital, and submandibular areas. The nasal bridge, eyelids [1], and forehead [2] have also been sites described. A linear form has also been reported [3]. There is a femal predominance and the condition generally develops in the forth to seventh decades [1]. Generally no etiological factor can be identified [1], although associations with local irritants, such as cosmetics, creams, perfumes, eye glasses, ionizing radiation, topical corticosteroids, benoxaprofen, and trauma have been reported [1]. In addition, some skin or internal diseases may be associated or present as MEP or MEP-like lesions. These include lupus erythematosous [4], lichen planus follicularis tumidus, sebocystomatosis, and psuedoxanthoma elasticum [5].
Bilaterally distributed retroauricular MEP has been reported only rarely (MEDLINE search) and the present case is the forth one [6, 7, 8]. These include two females (65- and 49-year-olds) and one male (45-year-old) with a duration of 12, 3, and <24 months respectively. The male patient also had MEP in the supraclavicular area. Infiltration of inflammatory cells was absent or only slightly present in all of these three patients. No specific etiological factor was identified in these patients [6, 7, 8].
Because of the limited number of reported MEP (about 30 cases) no single treatment has been proven to be more effective than others. We used simple extraction of the cysts and avoidance of topical irritants; in cases reported by other authors electrodessication, minocycline, topical tretinoin, and photodynamic therapy with ALA were also used and gave various results [1, 9, 10]. Of the three patients mentioned above, one refused the treatment, another failed to respond to topical tretinoin, and the third responded to topical tretinoin but recurred after discontinuation and an excision was later performed.
In summary we presented a very rare case of a young female with one-year history of bilateral retroauricular Milia en plaque in whom no etiological factor was identified and was managed with simple extraction of milia. A review of similar cases was also included.
References
1. Stefanidou MP, Panayotides JG, Tosca AD. Milia en plaque: a case report and review of the literature. Dermatol Surg2002 Mar;28(3):291-5. [PubMed]2. Fujita H, Iguchi M, Kenmochi Y, Fukunaga Y, Asahina A. Milia en plaque on the forehead. Journal of Dermatology2008;35(1):39-41. [PubMed]
3. Kautz O, Muller S, Braun-Falco M, Nashan D. Milia en plaque in a linear pattern. J Eur Acad Dermatol Venereol2009 Feb 27. [PubMed]
4. Belhadjali H, Youssef M, Yahia S, Njim L, Zakhama A, Zili J. Milia en plaque and discoid lupus erythematosus. Clin Exp Dermatol2009 May 16. [PubMed]
5. Tsoitis G, Papadimitriou C, Asvesti C, Lefaki J, Lambroudi M, Hatzibougias J, et al. [Retroauricular dermatitis of the "milia en plaque" type]. Ann Dermatol Venereol1993;120(1):58-64. [PubMed]
6. Le Guyadec T, Bosonnet S, Saint-Blancard P, Maccari F, Le Vagueresse R, Lanternier G. ["Milia en plaque" with multiple and successive localizations]. Ann Dermatol Venereol2000 Feb;127(2):208-9. [PubMed]
7. Calabrese P, Pellicano R, Lomuto M, Castelvetere M. Milia en plaque. J Eur Acad Dermatol Venereol1999 Mar;12(2):195-6. [PubMed]
8. Stork J. Retroauricular bilateral 'milia en plaque'. Dermatology1995;191(3):260-1. [PubMed]
9. Al-Mutairi N, Joshi A. Bilateral extensive periorbital milia en plaque treated with electrodesiccation. J Cutan Med Surg2006 Jul-Aug;10(4):193-6. [PubMed]
10. Keohane SG, Beveridge GW, Benton EC, Cox NH. Milia en plaque--a new site and novel treatment. Clin Exp Dermatol1996 Jan;21(1):58-60. [PubMed]
© 2010 Dermatology Online Journal