Multifocal tuberculosis revealed by multiple cutaneous gummas in the immunocompetent
Published Web Location
https://doi.org/10.5070/D32zs4d20kMain Content
Multifocal tuberculosis revealed by multiple cutaneous gummas in the immunocompetent
Mariem Bounouar1, Hanane BayBay1, Salim Gallouj1, Meriame Meziane1, Ouafae Mikou1, Fatimazahra Mernissi1, Meriem Chraibi2, Taoufik Harmouch2, Afaf Amarti2
Dermatology Online Journal 17 (5): 8
1. Department of Dermatology, Hassan II University Hospital, Fez, Morocco. bounouar.mariem@gmail.com2. Department of Pathology, Hassan II University Hospital, Fez, Morocco
Abstract
Cutaneous tuberculosis is rare. Its occurrence in multifocal tuberculosis (MT) is uncommon and happens frequently in the context of immunosuppression. We report the case of MT with multiple cutaneous gummas and bone and lung involvement that occurred in an apparently immunocompetent patient.
Case report
 |  |
| Figure 1 | Figure 2 |
|---|---|
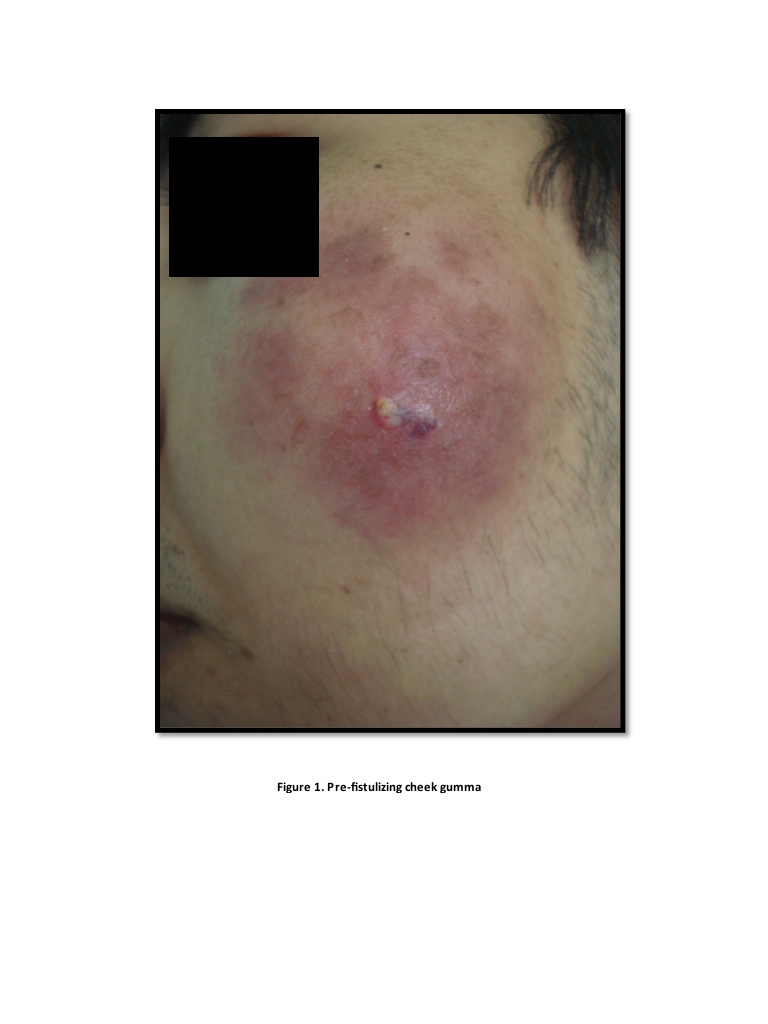
| Figure 1. Cheek gumma before fistula formation Figure 2. Ulcered gumma of ankle | |
 |  |
| Figure 3 | Figure 4 |
|---|---|
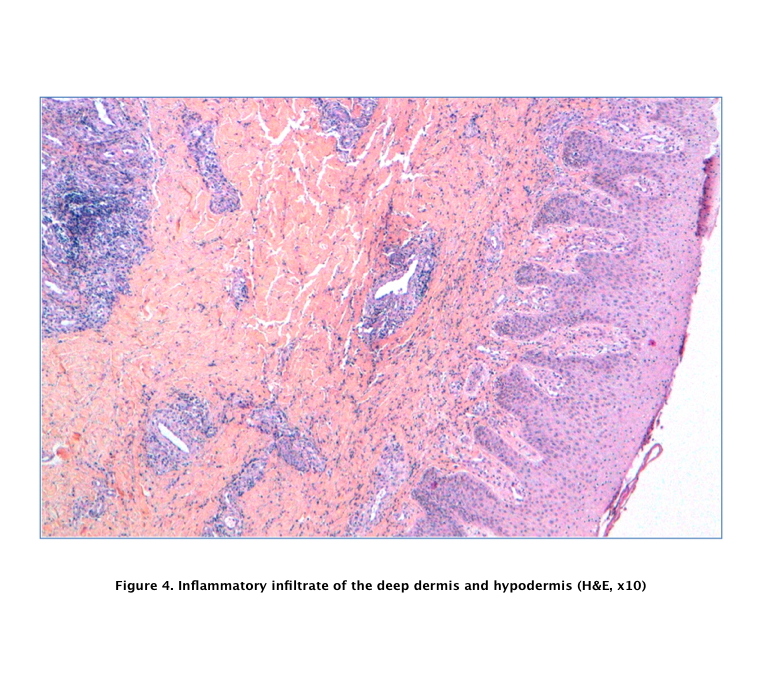
| Figure 3. Latero-sternal scrofulodermal gumma Figure 4. Inflammatory infiltrate (H&E, x10) | |
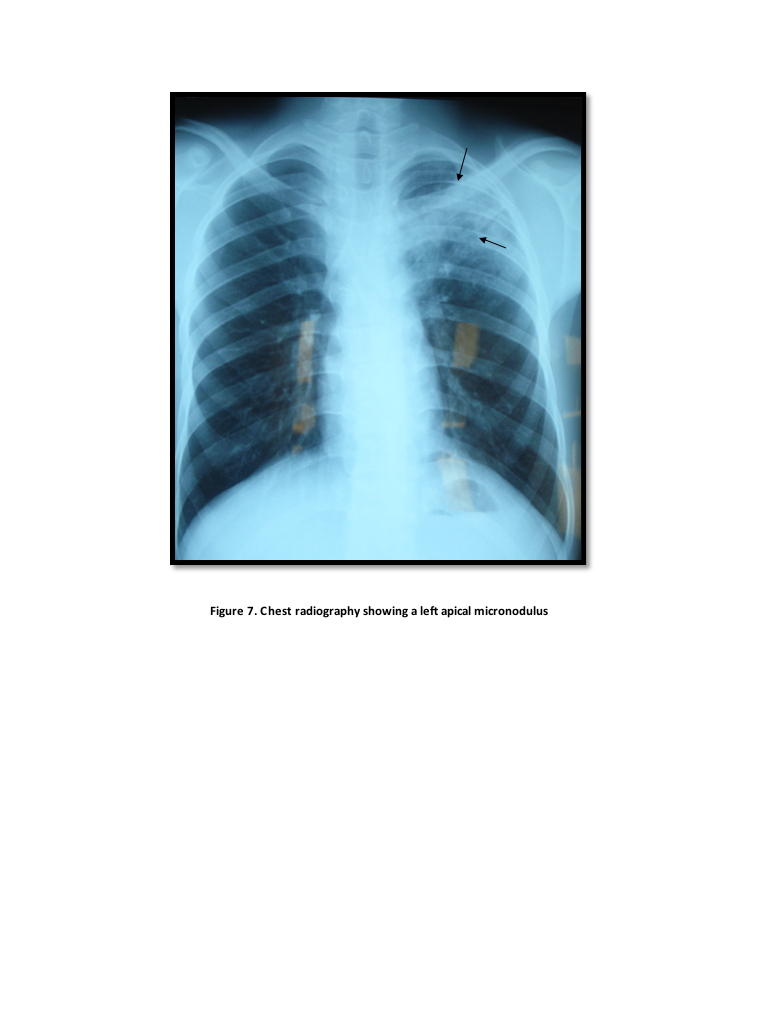
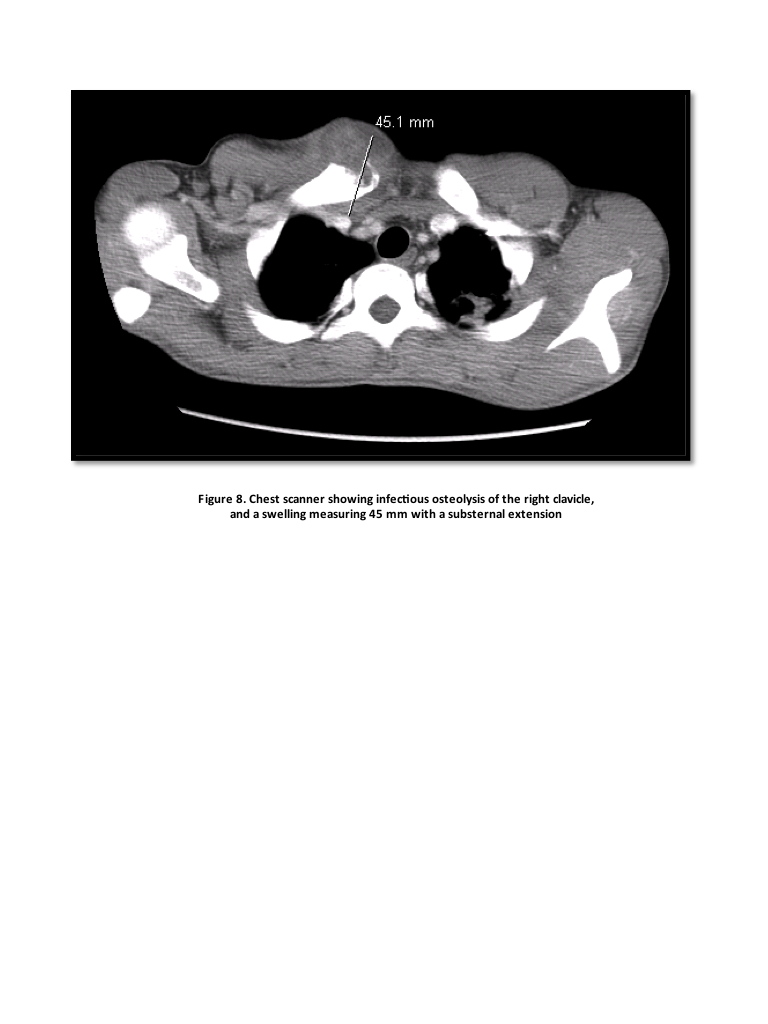
A 19-year-old man, without any known exposure to tuberculosis was hospitalized for multiple gummas at different stages (Figures 1, 2, and 3). Two episodes of hemoptysis with weight loss (10 kg in 2 months), fever and night sweats had been reported. The histology showed inflammatory infiltrate rich in neutrophils of the deep dermis and hypodermis without tuberculoid granuloma (Figures 4, 5, and 6). The intradermal tuberculin reaction and direct examination looking for resistant acid-alcohol bacillus in sputum, gastric fluid, and pus from gummas were negative. Culture on Löwenstein-Jensen, done with ulcerated skin lesions and bronchial washings, showed Mycobacterium tuberculosis. Chest radiography showed left apical micronodules (Figure 7) and CT chest showed apical excavated images, infectious osteolysis of the right clavicle, and a swelling measuring 45 mm with a substernal extension (Figure 8). Radiography of the right ankle was normal.
 |  |
| Figure 5 | Figure 6 |
|---|---|
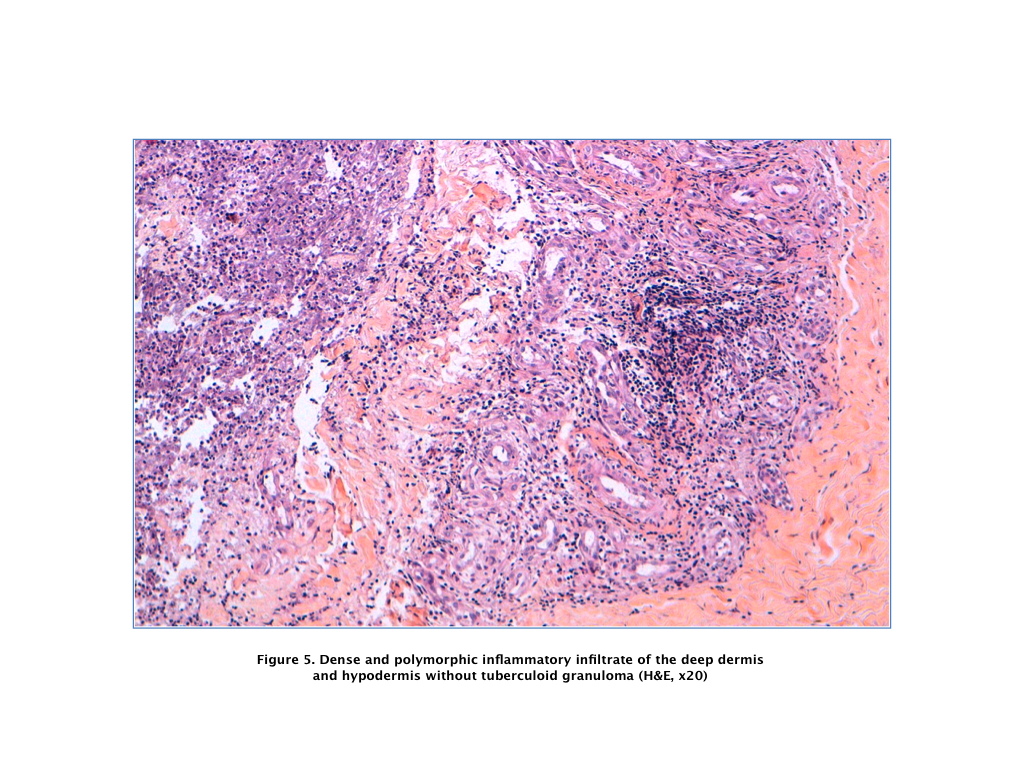
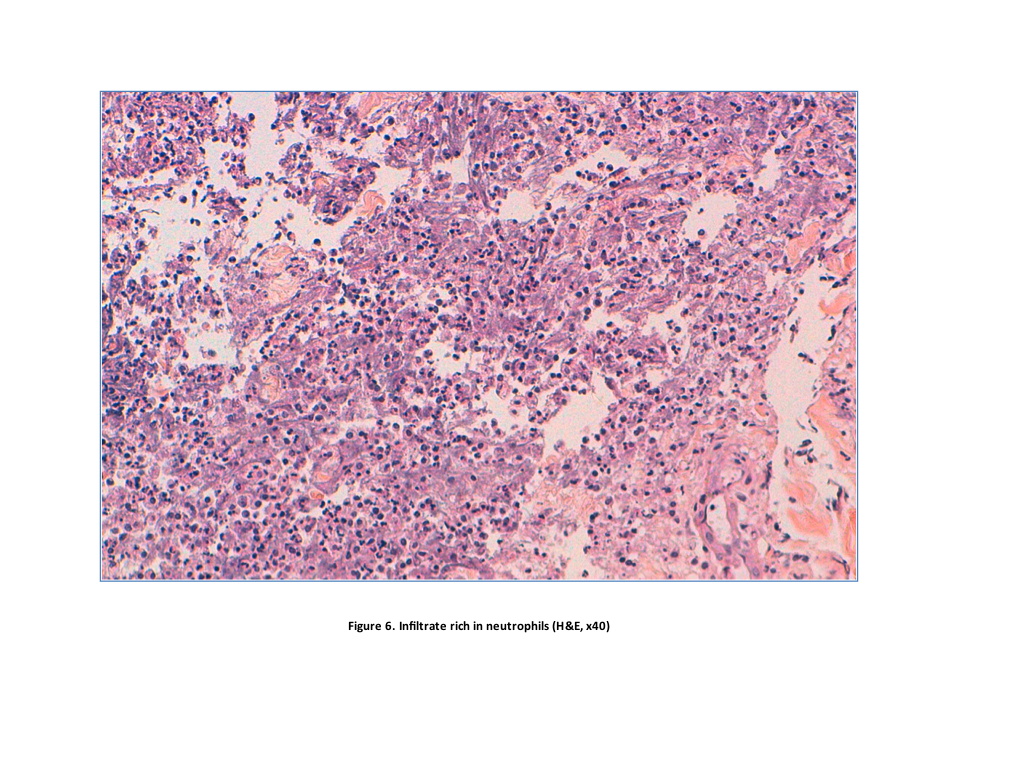
| Figure 5. Dense and polymorphic inflammatory infiltrate (H&E, x20) Figure 6. Infiltrate rich in neutrophils (H&E, x40) | |
 |  |
| Figure 7 | Figure 8 |
|---|---|
| Figure 7. Chest radiography showing left apical micronodules Figure 8. Chest CT scan showing infectious osteolysis of the right clavicle and a swelling measuring 45 mm with a substernal extension | |
This patient had no family history of tuberculosis and no particular susceptibility to tuberculosis in his ethnic group. He had no background of immunosuppression.. There was no history of diabetes, renal failure, or long-term treatment with corticosteroids or immunosuppressants; HIV serology and viral hepatitis were negative. He received antituberculosis therapy based on: ethambutol (20mg/Kg/24h), rifampicin (10mg/Kg/24h), isoniazid (5mg/Kg/24h), and pyrazinamide (25mg/Kg/24h) for two months, then rifampicin (10mg/Kg/24h) and isoniazid (5mg/Kg/24h) for seven months (2 ERIP / 7 RP).
The outcome was good with healing of skin lesions in six weeks and disappearance of radiological signs.
Discussion
In Morocco, where tuberculosis is a real public health problem, cutaneous tuberculosis occupies the fifth rank among the forms of extra-pulmonary tuberculosis [1]. Its occurrence in MT is uncommon and happens frequently in the context of immunosuppression. Multifocal forms of tuberculosis represent 9 to 10 percent of cases [2] and are confined mostly to immunocompromised patients especially with HIV infection. Their prognosis is poor with a mortality rate of 16 percent to 25 percent [3]. The diagnosis of MT is difficult because of the clinical polymorphism and the diversity of organs that can be involved. This is reflected in the typical delay in diagnosis of around 3 months [2, 3]. The skin represents an accessible organ to clinical and histological examination, which is helpful for diagnostic testing.
The common clinical forms of cutaneous tuberculosis are scrofuloderma and gummas. Widespread involvement in immunocompetent patients is rare and evaluation for underlying immunosuppression should be performed.
In fact, gummas are the result of hematogenous spread of bacilli from a visceral localization in a context of low immunity. The tuberculin test is often negative in these clinical forms [4]. In our patient, its negativity, despite the absence of laboratory evidence of immunosuppression, could be explained by moderate malnutrition (Body Mass Index equal to 18); the patient came from a disadvantaged socioeconomic environment.
The absence of granulomatous lesions in tuberculous gummas is possible but uncommon; tuberculoid granuloma is sometimes replaced by a non-specific inflammatory infiltrate of neutrophils [4].
Few observations of multifocal tuberculosis in the immunocompetent have been reported in the literature [5]; in these, skin involvement was even rarer. A special case has been reported in an immunocompetent 23-year-old, who presented with a tuberculous gluteal abscess with scrofuloderma and tubercular lymphadenitis [3].
Our patient presents two simultaneous forms of cutaneous tuberculosis: diffuse cutaneous gummas and scrofuloderma, resulting from direct extension of clavicular osteitis. He also exhibits a rare site of tuberculosis, which is the chest wall [6], that presented as a swelling next to the inner edge of the right clavicle.
We present a new case of multifocal tuberculosis, which is peculiar because of the combination of scrofuloderma and diffuse cutaneous gummas, revealing other foci of tuberculosis without an obvious context of immunosupression.
The resolution with antituberculosis therapy has been durable, with a current follow up of 19 months.
References
1. Ministère de la Santé Publique. Royaume du Maroc. Le nouveau programme national de lutte antituberculeuse; 1990.2. Soualhi M, Iraqi G, Belkheiri S, Zahraoui R, Chaibainou A, Benamour J et al. Multifocal tuberculosis (palpebral and pleural) in an immunocompetent woman. Rev Mal Respir. 2006 Jun;23(3 Pt 1):281-4. [PubMed]
3. Rai VM, Shenoi SD, Gowrinath. Tuberculous gluteal abscess coexisting with scrofuloderma and tubercular lymphadenitis.Dermatol Online J. 2005 Dec 1;11(3):14. [PubMed]
4. Morand JJ, Cuguillière A, Sayag J. Tuberculose cutanée. Encycl Méd Chir (Elsevier, Paris), Dermatologie, 98-360-A-10, 1999, 12 p.
5. Ben Abdelghania K, Mahfoudhia M, Turkia S, Bailia L, Dridia A, Khedera A. Tuberculose multifocale chez des sujets immunocompétents: deux cas. Rev Rhum 2006; 73 : 1122
6. Bouslama K, Bakir L, Ben M’rad S, Aloulou R, Hendaoui L, Ben Salah N, et al. Tuberculose de la paroi thoracique: à propos d'un cas et revue de la littérature. Méd Mal Infect. 1998; 28 : 666-667.
© 2011 Dermatology Online Journal