Sorafenib-associated remission of psoriasis in hypernephroma: Case report
Published Web Location
https://doi.org/10.5070/D32z47h80wMain Content
Sorafenib-associated remission of psoriasis in hypernephroma: Case report
Christa Fournier, Glenn Tisman MD
Dermatology Online Journal 16 (2): 17
Glenn Tisman, M.D. A Medical Corporation, Whittier, California. christa324@gmail.comAbstract
Psoriasis is a disease characterized by epidermal hyperproliferation that results in the formation of lesional plaques covered by scale. Psoriasis is thought to be angiogenesis dependent. Clear cell renal cell carcinoma is a hypervascularized solid tumor associated with loss of function of the von Hippel-Lindau (VHL) tumor suppressor gene and increased Raf-1 activity. A 68-year-old man who suffered from recalcitrant psoriasis for over 50 years was treated with sorafenib for metastatic clear cell renal carcinoma. One month later, his psoriasis, previously 8 x 6 cm on the mid posterior thorax, completely resolved. Sorafenib works by inhibiting several receptor tyrosine kinases (RTKs), such as vascular endothelial growth factor (VEGFR) and platelet-derived growth factor receptor (PDGFR)). It also inhibits intracellular Raf kinase (Raf-1), which targets the ubiquitous mitogen-activated protein kinase (MAPK) intracellular signal transduction pathway. We suggest that this patient’s remission of psoriasis could be related to the inhibition/modulation of VEGF, PDGFR, Raf-1, and MAPK.
Introduction
 |
| Figure 1 |
|---|
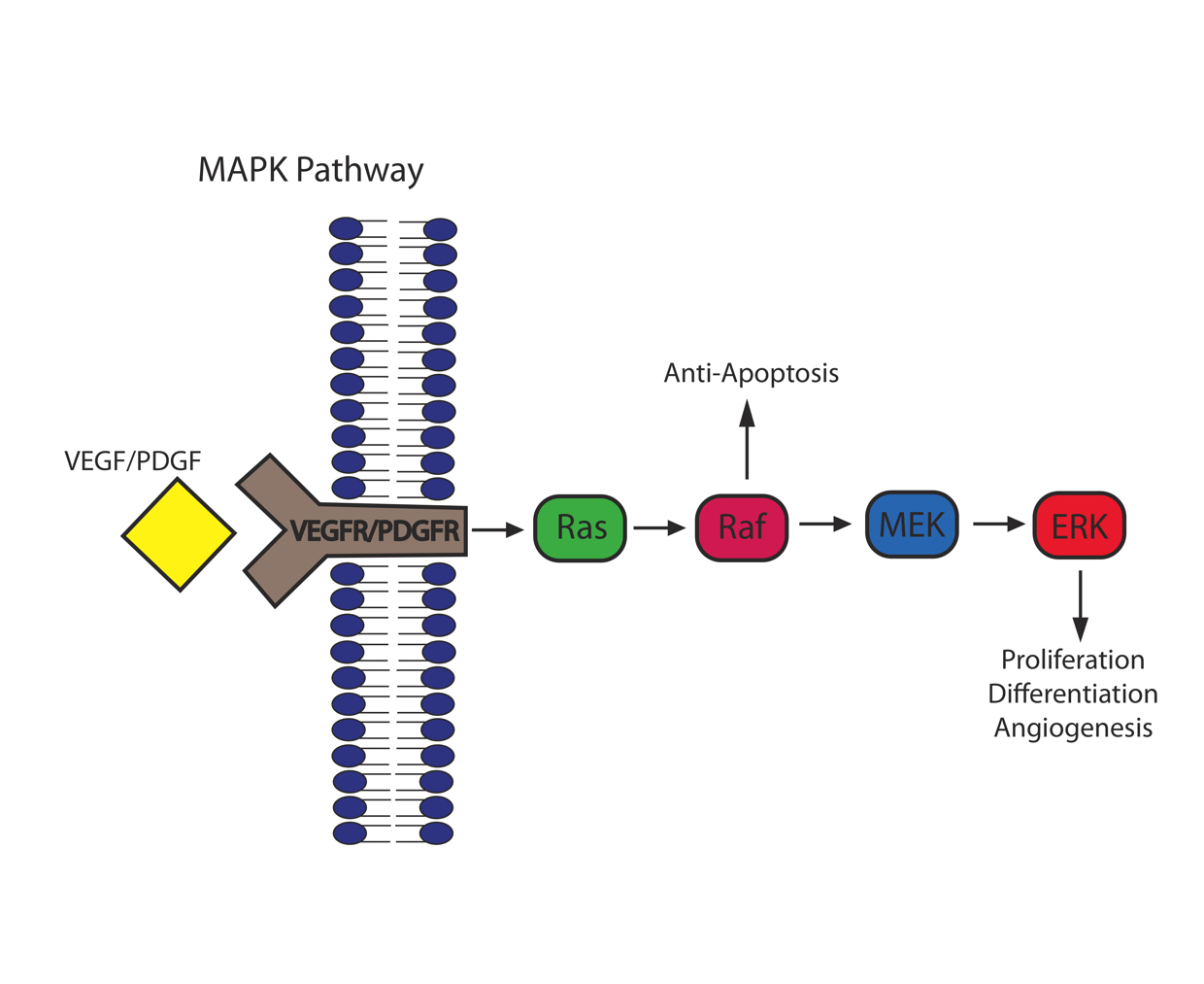
| Figure 1. MAPK Pathway |
Angiogenesis primarily occurs in early life to establish adequate vasculature and thereby support growth and embryonic development. Very little endothelial cell turnover occurs in adults and is limited to the ovarian cycle and the wound healing process. Angiogenesis occurs when growth factors induce signaling via their respective receptor tyrosine kinases (RTKs), on the surface of endothelial cells and/or pericytes, followed by activation of the ubiquitous mitogen-activated protein kinase (MAPK) intracellular singal transduction pathway. This highly conserved pathway comprises Raf kinase, mitogen extracellular kinase (MEK), and extracellular signal-regulated kinase(ERK). The pathway results in cell proliferation, mobility, survival and angiogenesis [1]. Figure 1 shows the MAPK pathway.
Psoriasis is a disease characterized by the presence of symmetrical, well-demarcated, erythematous plaques covered by scale [2]. There is epidermal hyperproliferation and abnormal keratinization, inflammation, and local vascular changes with activated endothelial cells [3]. Psoriasis is primarily a lymphocyte driven disease. However, the prominence of dermal microvascular expansion in lesional skin suggests that psoriasis is angiogenesis-dependent. A central feature of angiogenesis in psoriatic lesions is the presence of increased endothelial cell proliferation [2].
Keratinocytes in lesional skin have been found to be a major source of pro-angiogenic cytokines in psoriasis. Several angiogenic factors have been identified including interleukin-8, tumor necrosis factor-alpha (TNF-alpha), transforming growth factor-alpha (TGF-alpha), endothelial cell stimulating angiogenesis factor, thymidine phosphorylast (TP), and vascular endothelial growth factor (VEGF) [2]. Detmar et al. demonstrated increased VEGF mRNA production in lesional psoriatic keratinocytes and reported upregulation of VEGF receptors (VEGFR-1 and VEGFR-2) on lesional psoriatic microvasculature [4]. Platelet-derived growth factor receptor (PDGFR) has been found to have increased expression in dermal fibroblasts and in dermal blood vessels of psoriatic lesions. In normal skin, PDGFR is expressed at low levels [5].
A study by Haase et al showed that activation of mitogen-activated protein kinase (MAPK) in basal and suprabasal keratinocytes of human psoriatic lesions correlated with suprabasal integrin expression. In normal epidermis, integrin expression is confined to the basal layer and MAPK activation is not present. They proposed that the activation of MAPK, either directly or indirectly through increased IL-1α production, is responsible for epidermal hyperproliferation in psoriasis [6].
Clear cell renal cell carcinoma (RCC) is the most prevalent and aggressive histological type of renal cancer. It is associated with the loss of function of the von Hippel-Lindau (VHL) tumor suppressor gene. Loss of VHL function results in hypoxia inducible factors (HIF1 and HIF-2, and subsequent overexpression of proangiogenic (e.g. VEGF) and autocrine growth factors (e.g. TGF-α) [1].
Clear cell RCC is a hypervascularized solid tumor also associated with increased Raf-1 activity. Studies have shown that TGF-α is overproduced in mice lacking the VHL gene. TGF-α binds to the EGFR of tumor cells to initiate an autocrine growth loop that involves HIF-2 upregulation, increased VEGF production, and tumor angiogenesis. VEGF is a tumor-secreted cytokine with critical importance in both normal and tumor-induced angiogenesis. It results in the activation of the MAPK pathway (RAS/RAF/ERK) signaling pathway, which is involved in regulation of endothelial apoptosis and angiogenesis [1].
In this case report, the patient had suffered from psoriasis for over 50 years until he was treated with sorafenib for metastatic renal cell carcinoma, a tumor that is characteristically associated with increased vascularity. Here, we present the serendipitous observation of complete remission of resistant psoriasis during therapy for metastatic renal cell cancer induced by sorafenib.
Case presentation
The patient is a 78-year-old man who was diagnosed with psoriasis in 1952 when he was 22 years old. He initially had psoriatic plaques only on his scalp, but gradually lesions involved his neck and upper back.
The patient received topical steroids and phototherapy, with little relief. Eventually, he was able to control outbreaks with daily topical betamethasone dipropionate. He noticed that alcohol consumption caused lesions to flare. When he abstained from alcohol, he experienced fewer outbreaks.
The patient was diagnosed with hypernephroma in 2000 at age 69, after having a right nephrectomy due to a renal mass. A 13.2 cm renal cell carcinoma that was clear cell type and had a nuclear Grade III was identified. Three perinephric pelvic lymph nodes were positive for metastatic disease. Eight years later, he presented with right shoulder pain, right scapular mass and a 1 cm calcified bone lesion that was identified in the proximal shaft of the humerus. Biopsy revealed moderately to poorly differentiated Grade III renal cell carcinoma. The patient was also found to have a pancreatic head mass with a normal CA 19-9 titer (13.2 units/mL) and a hepatic lesion both representing metastatic hypernephroma.
Prior to treatment for the hypernephroma, the patient had a psoriatic plaque that measured 8 x 6 cm and was positioned over the mid posterior thorax. The patient was started on sorafenib 200mg twice daily by mouth on August 15, 2008. Two-and-a-half weeks later, the chronic psoriatic lesions were noted to have dramatically regressed. One month after beginning sorafenib, the lesions completely regressed. As of December 2008, the patient was free of psoriatic lesions and he no longer complained of itching and sensitivity. No other psoriatic therapy or change in lifestyle occurred during this time.
The patient had a mixed tumor response to sorafenib. There was a slight interval decrease in size of the pancreatic head mass after being on sorafenib for three months. However, there was no decrease in size of the metastatic scapular lesion or the hepatic lesion.
After the patient's hypernephroma became resistant to sorafenib, he was changed to sunitinib therapy and the psoriatic plaque reappeared after approximately one month. In addition, sunitinib induced another partial remission of his hypernephroma. He is currently resistant to sunitinib and will be changing therapy again soon. His psoriatic plaque remains to this day.
Discussion
Sorafenib (BAY 43-9006) is a novel bi-aryl urea developed by BAYER Pharmaceutical Corporation and Onyx to target the MAPK pathway (i.e., Raf/MEK/ERK) by acting as a potent Raf-1 inhibitor in tumor cells. Sorafenib binds to Raf kinase and stabilizes the protein in an inactive conformation. Several RTKs have also been found to be inhibited by sorafenib, including VEGFR-1/-2/-3, PDGFR-B, c-Kit, Flt-3, and RET [1].
In psoriasis, PDGFRs are overexpressed and keratinocytes produce pro-angiogentic cytokines including VEGF. These VEGFs stimulate the VEGFRs, which activates Ras and the MAPK pathway (Raf/MEK/ERK) and inhibits cell proliferation and angiogenesis. We suggest that sorafenib disrupts this pathway in psoriatic skin just as it does in renal cell carcinoma. By inhibiting VEGFR, PDGFR, and/or Raf-1, angiogenesis is downregulated.
We propose that inhibition by sorafenib of the known mechanisms of angiogenesis that are shared by the psoriatic process and the increased supportive vascularity characteristic of hypernephroma is responsible for the synchronous partial tumor response observed in the patient and the complete resolution of psoriasis. Further study of sorafenib and similar acting drugs may uncover drugs of value for the control of psoriasis. Likewise, therapies effective for psoriasis may have value in the therapy of hypernephroma.
References
1. Voliotis D, Dumas J. Clinical development of sorafenib (BAY 43-9006), a VEGFR and RAF inhibitor. In Tumor Angiogenesis: Basic Mechanisms and Cancer Therapy. Part 4. Edited by Marme D & Fusenig N. New York: Springer Berlin Heidelberg; 2008:655-671.2. Creamer D, Sullivan D, Bicknell R, Barker J. Angiogenesis in psoriasis. Angiogenesis. 2002;5:231-236. [PubMed]
3. Guenther LC, Ortonne JP: Pathophysiology of psoriasis: science behind therapy. J Cut Med Surg. 2002;6:2-7. [PubMed]
4. Detmar M, Brown LF, Claffey KP, et al. Overexpression of vascular permeability facto/vascular endothelial growth facto and its receptors in psoriasis. J Exp Med 1994;180:1141-1146. [PubMed]
5. Krane JF, Murphy DP, Gottleib AB, et al. Increased dermal expression of platelet-derived growth factor receptors in growth-activated skin wounds and psoriasis. J of Invest Derm. 1991;96:983-986. [PubMed]
6. Haase I, Hobbs RM, Romero MR, et al. A role for mitogen-activated protein kinase activation by integrins in the pathogenesis of psoriasis. J Clin Invest. 2001;108:527-536. [PubMed]
© 2010 Dermatology Online Journal