Keratoacanthoma centrifugum marginatum arising in vitiligo: A case report
Published Web Location
https://doi.org/10.5070/D32rp0c8nhMain Content
Keratoacanthoma centrifugum marginatum arising in vitiligo: A case report
Dr Sasi kiran Attili MRCP1, and Dr V Ratnam Attili MD2
Dermatology Online Journal 12 (2): 18Key Words: Keratoacanthoma Centrifugum Marginatum, Vitiligo, Methotrexate, Discoid Lupus
Erythematosus.
1. Department of Dermatology/Photobiology, Ninewells Hospital & Medical School, Dundee. skattili@hotmail.com2. Visakha Institute of Skin & Allergy, Visakhapatnam, India
Abstract
Keratoacanthoma centrifugam marginatum (KCM) is a rare variant of the Keratoacanthoma (KA) form of squamous cell carcinoma with only 30 cases reported to date. We report a case of KCM arising in a long-standing vitiligo lesion chronically exposed to sunlight. Over years, the vitiligo lesions gradually evolved into sclerotic plaques and subsequently KCM developed in one of the plaques.
Introduction
Keratoacanthoma (KA) is a fairly common neoplasm among light-skinned people. Once considered a pseudomalignancy that resembled squamous cell carcinoma, it is now considered to be a cancer that resembles a pseudo-benign tumor [1]. Males are affected three times more often than females and epidemiological data suggests that the incidence is related to sun exposure [2]. In most cases, the tumor presents as a solitary lesion. Several variants of KA with multiple lesions and three rare variants of solitary KA have been described: subungual KA, giant KA, and keratoacanthoma centrifugam marginatum (KCM). The last two forms attain large sizes. The giant KA spreads vertically downwards destroying the underlying tissues and KCM spreads horizontally across the surface reaching a size of 20cm or more. Unlike the solitary KA, KCM shows no tendency toward spontaneous resolution. Instead, there is peripheral extension with a raised, rolled border and atrophy in the center of the lesion [3].
KA is not common in dark skinned people [4]. We present here a KCM lesion developing in a dark-skinned elderly Indian woman within a vitiligo patch exposed to sun light over many years.
Clinical synopsis
 |  |
| Figure 1a | Figure 2a |
|---|
A 65-year-old woman, in good health, presented with a rapidly growing plaque over her right forearm (Fig. 1a). The tumor appeared around 3 months earlier, in an existing depigmented and sclerotic plaque of several years' duration (Fig. 2a). She was seen 10 years earlier in our clinic for white patches on her arms and trunk. A biopsy was not taken at that time, but clinically vitiligo with secondary actinic change or chronic discoid lupus erythematosus (DLE) had been considered. She was lost for further followup, until the recent spreading tumor appeared.
 |
| Figure 3a |
|---|
Examination revealed several large vitiliginous patches over her arms, chest, upper back, midriff, and periungual areas, all predominantly in sun exposed areas (Fig. 3a). She had no lesions on her face or scalp. Remarkably, the lesions on her upper limbs showed clear evolution as they progressed distally (Fig. 2a). Erythema, palpable sclerosis and fine scaling on the surface were more marked, as the degree of sun-exposure increased (i.e., from proximal to distal). The tumor under consideration was a large verrucous growth on her right forearm about 8 × 5cm in size, with rolled, elevated margins and an irregular surface with tiny ulcerations. The tumor had a firm feel, was free from the underlying structures, non-tender, and did not bleed to touch. There was no regional lymphadenopathy. All her baseline investigations including full blood count, renal and liver function tests were normal.
 |
| Figure 1b |
|---|
Biopsies were taken from the margin of the verrucous growth, from an adjacent inflammatory sclerotic lesion, and from a macular vitiligo lesion on the upper arm.
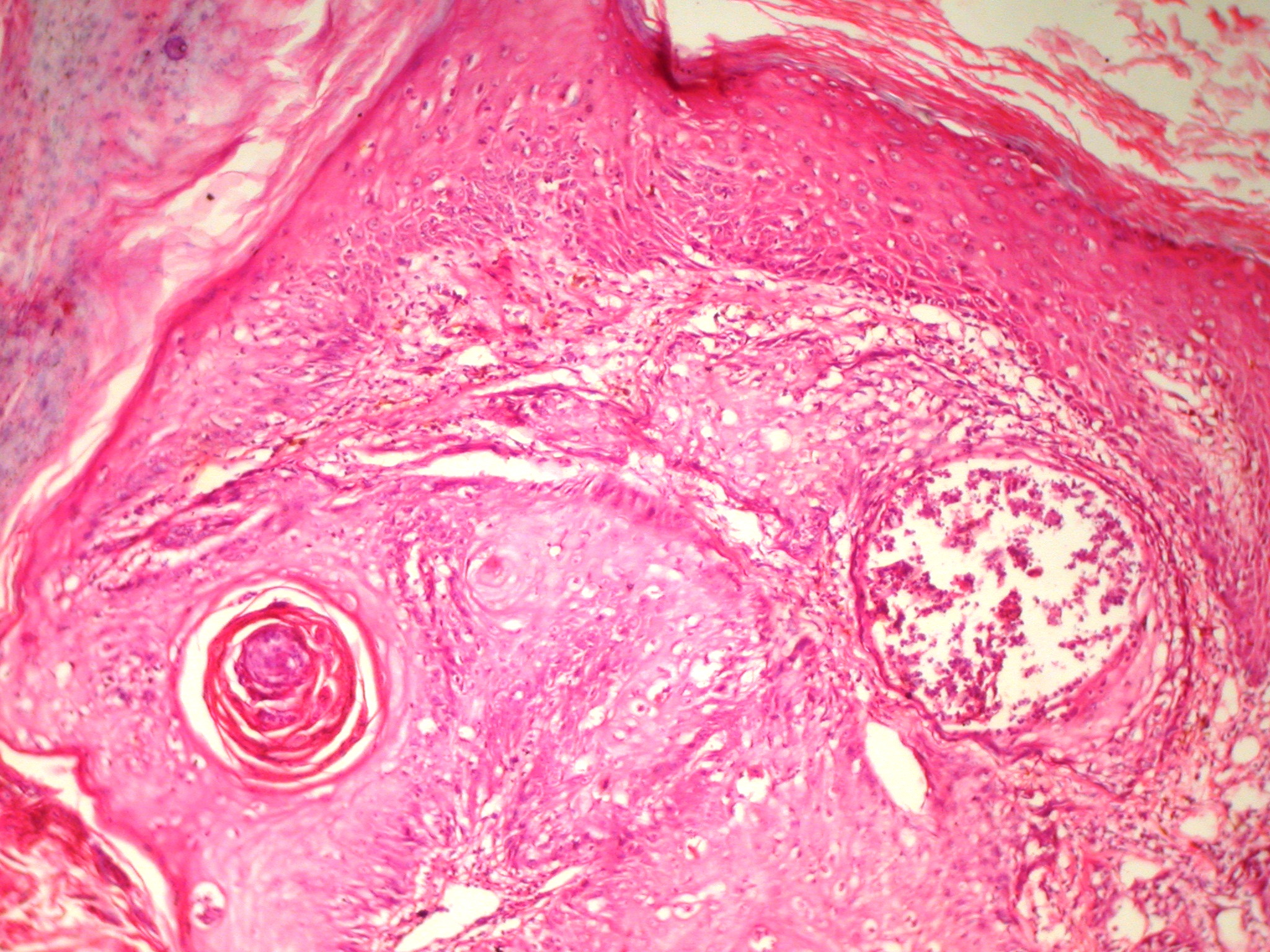
Histopathology of the verrucous growth (Fig. 1b) showed pseudoepitheliomatous hyperplasia composed of lobules of mature squamous epithelium with pale cells and mild cytological atypia. Keratinization and cyst formation were prominent and mitotic figures were rare. In the surrounding dermis, a mild to moderate mononuclear cell infiltrate was present.
 |  |
| Figure 2b | Figure 3b |
|---|
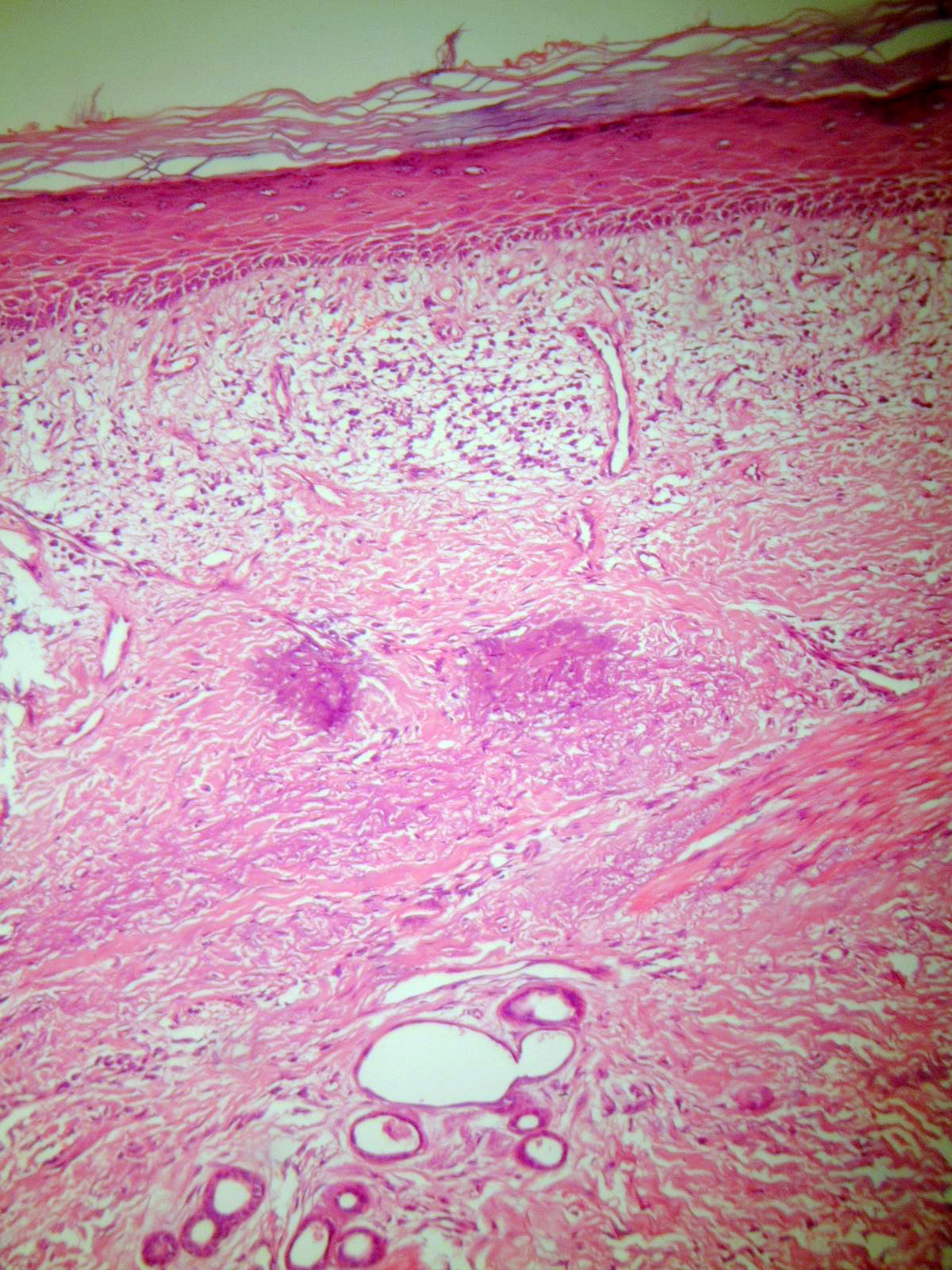
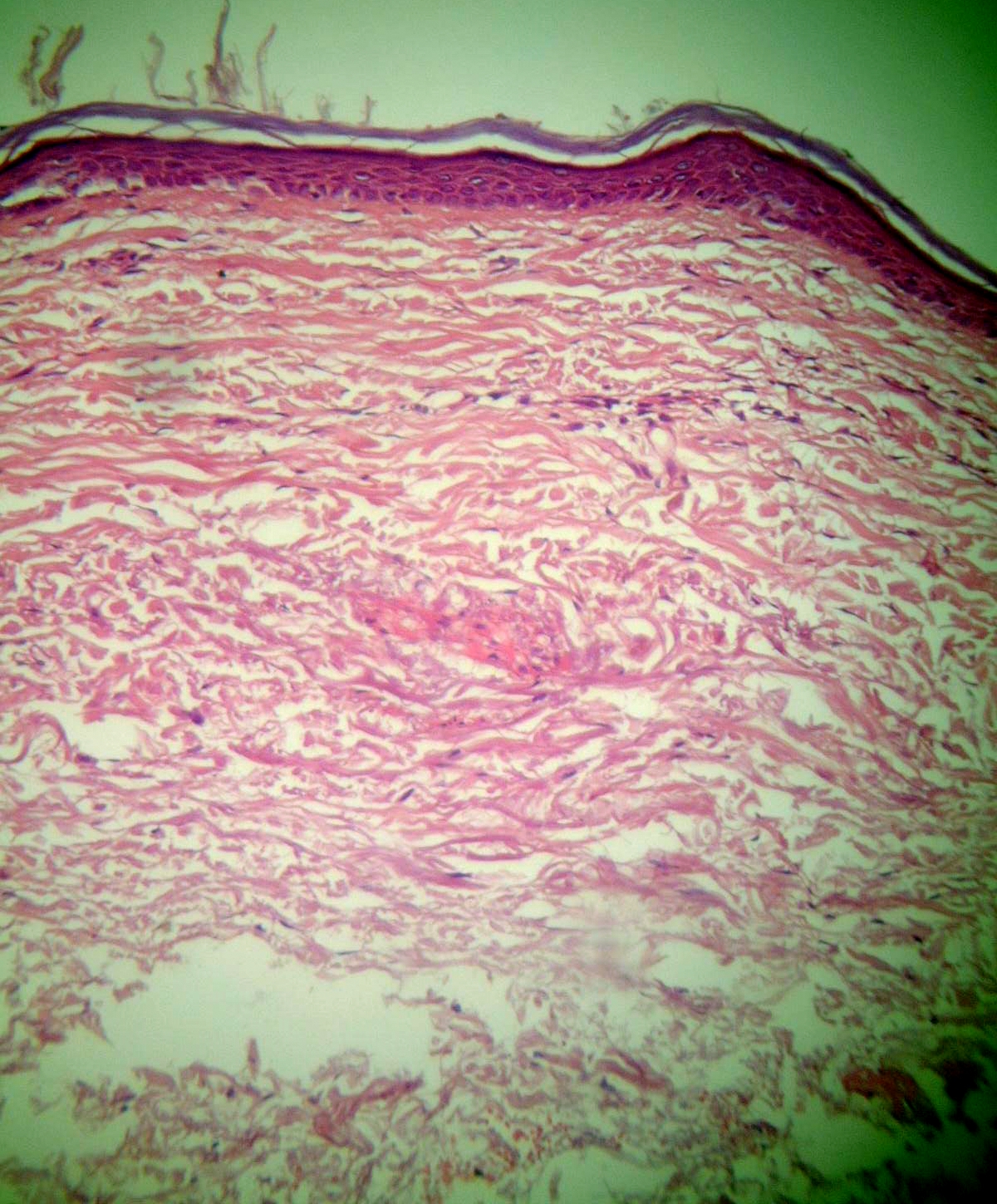
The inflammatory sclerotic plaque (Fig. 2b) showed a dense band of upper dermal lichenoid infiltrate with basal layer degeneration. The dermis showed significant fibrosis and solar elastosis. A thin, flat epidermis and absence of melanocytes characterized the macular vitiligo lesion (Fig. 3b). There were no significant inflammatory cells in the dermis.
 |
| Figure 4 |
|---|
| KCM after treatment |
Considering the clinical and histological features, our diagnosis was KCM arising in chronically sun-exposed skin; the presence of long-standing, relatively inactive DLE could not be ruled out.
The KCM lesion regressed considerably over a 2-month period while being treated with methotrexate (25 mg intramuscular weekly) and topical applications of trichloroacetic acid. Once the tumor decreased to 3 × 2 cm it was resistant to further methotrexate therapy, but resolved completely after electrodesiccation and curettage. The lesional skin regained its original sclerotic appearance (Fig. 4). The patient is currently under followup. No new KCM lesions have appeared nor has there been any recurrence in the last 3 years. The chronic plaques have remained stable.
Discussion
This case had several unusual features. Gradual transformation of vitiliginous patches to sclerotic scaly plaques in maximally sun exposed areas suggested a diagnosis of chronic and stable vitiligo with secondary actinic changes and possible transformation to DLE. The histological features of a band like lichenoid infiltrate with dermal fibrosis in the inflammatory sclerotic plaques did not solve the clinical enigma. Disseminated morphea was also considered possible. Few cases of vitiligo in association with morphea [5] and also DLE have been reported [6].
A verrucous form of DLE has also been reported [7]. However, with the large size and rapidly spreading nature of the tumor in our patient, KCM was more likely to be the correct diagnosis. Spontaneous resolution of KA is usually associated with an intense lichenoid reaction. It is interesting that in our patient KCM developed in a plaque, which initially had an intense lichenoid reaction and after complete resolution regained its original plaque-type appearance without much evidence of scarring. Squamous cell carcinoma arising in chronic DLE has been reported [8]. Our case represents KCM developing in a patch of chronically sun-exposed vitiligo. The presence of DLE in the plaque preceeding the development of KCM could not be ruled out. KCM is generally known to be resistant to many therapies; our patient responded to methotrexate and curettage with electrodesiccation.
Acknowledgment: We are grateful to Dr. E.J.Calonje, Director of dermatohistopathology, St. John's Hospital for skin diseases, London, for reviewing the case notes and his opinion on the histopathological features.
References
1. Schwartz RA. Keratoacanthoma: A clinico-pathologic enigma. Dermatol Surg. 2004;30:2, Part 2, 326-3332. MacKie RM. Epidermal skin tumors. In: Rook/ Wilkinson/ Ebling's Textbook of Dermatology. 6th Edn. Vol.2. Blackwell Scientific Publications.1998:1662-1666.
3. Nigel Kirkhum. Tumors and cysts of the epidermis. In: Lever's Histopathology of the Skin. 8th Edn. Philadelphia: Lippincott-Raven Publishers. 1997:731-734.
4. Sullivan JJ. Keratoacanthoma: the Australian experience. Australs J Dermatol. 1997; 38(Suppl): S36-S39.
5. Saihan EM, Peachy DG. Vitiligo and Morphoea. Clin Exp Dermatol. 1979; 4:103
6. Choudhry DS. Development of Discoid lupus erythematosus in Vitiligo. Bull Calcutta Sch Trop Med. 1968; 16:111-112.
7. Uitto J, Santa-Cruz DJ, Eisen AZ et al. Verrucous lesions in patients with Discoid lupus erythematosus. Br J Dermatol. 1978;98:507
8. De Barker D,Dissaneyika M Burge S. The sequelae of chronic cutaneous lupus erythematosus. Lupus 1992; 1:181.
© 2006 Dermatology Online Journal