Clear cell papulosis
Published Web Location
https://doi.org/10.5070/D32kq6b3mkMain Content
Clear cell papulosis
Rachel Farley-Loftus MD, Nicole M Bossenbroek MD, Karla Rosenman MD, Julie V Schaffer MD
Dermatology Online Journal 14 (10): 19
Department of Dermatology, New York UniversityAbstract
A 2-year-old boy presented with multiple, hypopigmented, flat-topped papules in the pubic region and on the abdomen in a distribution pattern that followed the milk lines. The lesions had first appeared at age three months and increased in number over time. Histopathologic examination showed large clear cells within the lower epidermis, which stained positively with periodic acid-Schiff. These findings were diagnostic of clear cell papulosis, a rare condition that primarily affects young children. We review the histopathologic and immunohistochemical findings that link clear cell papulosis to clear cells of Toker and extramammary Paget disease.
 |  |
| Figure 1 | Figure 2 |
|---|
History
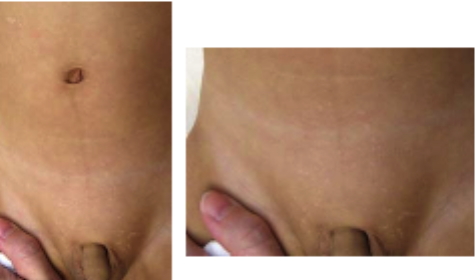
A healthy 2-year-old boy presented to the Pediatric Dermatology Clinic at Bellevue Hospital Center in October, 2007, for evaluation of an asymptomatic, hypopigmented eruption on the abdomen and in the pubic area. His parents initially noticed a few white spots superior to the scrotum at age three months and the lesions progressively increased in number and spread onto the abdomen. There was no family history of a similar eruption.
Physical Examination
Multiple (>50), barely-elevated, flat-topped, hypopigmented papules were grouped symmetrically in the pubic area and on the lower part of abdomen. Similar papules were present in a linear array on the right upper part of the abdomen; the overall distribution pattern followed the "milk lines." The individual lesions were round-to-polygonal in shape and measured 1- to 3-mm in diameter.
Lab
None.
Histopathology
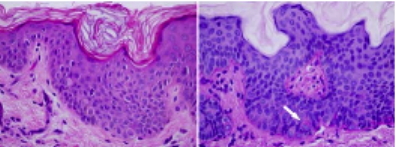
There are multiple enlarged epithelioid cells scattered throughout a slightly acanthotic and papillomatous epidermis. The cells have abundant pale staining cytoplasm, which reacts positively with a periodic acid-Schiff stain. Nuclear atypia and pleomorphism are absent.
Comment
Clear cell papulosis (CCP) presents with multiple, minimally-elevated, hypopigmented papules that are characterized histopathologically by clear cells within the lower portion of the epidermis. This condition was first described in 1987 and a total of 18 patients have been reported [1, 2, 3]. Most of the affected individuals were Asian (Taiwanese, Singaporean, Korean, or Indian), similarly, our patient was of Chinese heritage. A few cases of CCP were reported in Hispanic or Italian patients. The occurrence of CCP in three pairs of siblings suggests that genetic factors may have a role in its pathogenesis. Onset is typically during early childhood (mean, 1.7 years; range, 4 months to 6 years), with a single case identified in an adult [1, 2, 3]. The eruption favors the pubic region, lower abdomen, and other sites along the milk lines, which extend from the upper medial thighs to the anterior axillae. Involvement of the lower back and buttocks also has been observed [2, 3].
Histopathologic examination shows mild acanthosis, decreased epidermal pigmentation, and the presence of large clear cells singly or in small clusters within the basal and (occasionally) suprabasal layers of the epidermis [1]. These cells have abundant, clear cytoplasm and round or oval, pale nuclei that are sometimes grooved. They exhibit positive staining for epithelial membrane antigen (EMA), carcinoembryonic antigen (CEA), cytokeratin 7 (CK7), and anti-cytokeratin antibodies AE1/AE3. This pattern is identical to that of extramammary Paget disease and (with the exception of weaker CEA staining) of clear cells of Toker [1, 2, 3, 4]. Mucin stains (e.g., alcian blue, mucicarmine, and periodic acid-Schiff) are variably positive in CCP. In contrast, these stains are consistently positive in Paget disease and negative in Toker cells.
Toker cells, which have clear-to-pale-staining cytoplasm, can be identified within the lower epidermis in approximately 80 percent of normal nipples, 65 percent of accessory nipples, and 35 percent of vulvectomy specimens when immunohistochemical stains (e.g., CK7) are utilized [4]. The Toker cell has been characterized as a glandular epithelial cell that occurs at the interface between the epidermis and lactiferous ducts of the breast or ducts of mammary-like glands of the vulva. Toker cells, CCP, and Paget disease may therefore exist on a biologic continuum and represent a component of normal epidermis along the milk lines, a benign proliferation, and the result of malignant degeneration, respectively [3]. Multifocal Toker cell hyperplasia in association with primary intraepidermal mammary Paget disease has been described and hypo- or depigmentation is clinically evident in as many as 30 percent of cases of extramammary Paget disease [5]. Although long-term follow-up of CCP has not yet been reported, spontaneous regression has been postulated based on the relative paucity of observations of this condition in older children and adults [2].
References
1. Kuo TT, et al. Clear cell papulosis of the skin. Am J Surg Pathol 1987; 11: 827 PubMed2. Lee JY, et al. Clear cell papulosis of the skin. Br J Dermatol 1998; 138: 678 PubMed
3. Benouni S, et al. Clear cell papulosis in Hispanic siblings. Arch Dermatol 2007; 143: 358
4. Willman JH, et al. Vulvar clear cells of Toker: precursors of extramammary Paget's disease. Am J Dermatopathol 2005; 27: 185 PubMed
5. Yang CC, et al. Depigmented extramammary Paget's disease. Br J Dermatol 2004; 151: 1049 PubMed
© 2008 Dermatology Online Journal