An ulcerated tumor in an infant
Published Web Location
https://doi.org/10.5070/D32d84b29tMain Content
An ulcerated tumor in an infant
Sara Lotfi MD1, Fariba Ghalamkarpour MD2, Hoda Rahimi MD1, Zahra Asadi Kani MD3, Maryam Yousefi MD4, Mehdi Qaisari MD1
Dermatology Online Journal 16 (4): 9
1. Dermatology Resident2. Associate Professor of Dermatology
3. Dermatopathologist
4. Assistant Professor of Dermatology. myousefi_md@yahoo.com
Skin Research Center, Shahid Beheshti University Shohada-e Tajrish Hospital, Tehran, Iran
Abstract
Cutaneous leiomyoma is a benign dermal tumor of smooth muscle. Leiomyoma can occur at any age but typically develops during adolescence or early adult life. Congenital leiomyoma is an extremely rare reported variant. A five-month-old boy presented to our clinic with a progressively enlarging mass on his occipital scalp. Microscopic examination of the solitary ulcerated nodule showed a non-encapsulated mass in the dermis composed of spindle-shaped cells. The diagnosis was confirmed by immunohistochemical studies, which were compatible with leiomyoma. Therefore, clinical suspicion of leiomyoma should be considered in the case of a solitary ulcerated nodule in an infant.
History
A five-month-old boy presented to our clinic with a progressively enlarging mass on his occipital scalp. The lesion had been noticed one week after birth as a papule measuring 0.5 x 0.5 cm that gradually enlarged and ulcerated. The infant had a history of sepsis and respiratory distress syndrome at birth, but since then he had had no history of any other medical problems or trauma to the site. His parents were non-consanguineous. Family history was negative for similar conditions.
Physical examination
 |
| Figure 1 |
|---|
A 2 x 3 x 0.5 cm smooth, firm, non-tender, pink and semi-mobile mass with central ulceration and crust that wasn’t tender on touch was present on the occipital scalp (Figure 1). Systemic examination including lymph nodes revealed no abnormalities. Otherwise, the infant was healthy.
Laboratory data
Complete blood count and biochemistry tests were within normal ranges. Skull X-ray and triphasic bone scan showed no bone involvement. The lesion was totally excised and after a 6-month follow-up, the patient had no evidence of recurrence in the excision site.
Histopathology
 |  |
| Figure 2 | Figure 3 |
|---|
 |
| Figure 4 |
|---|
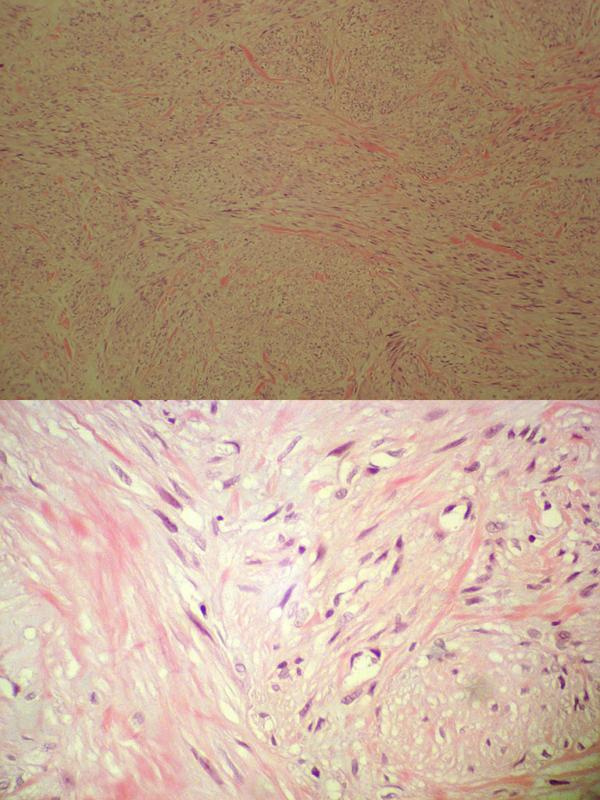
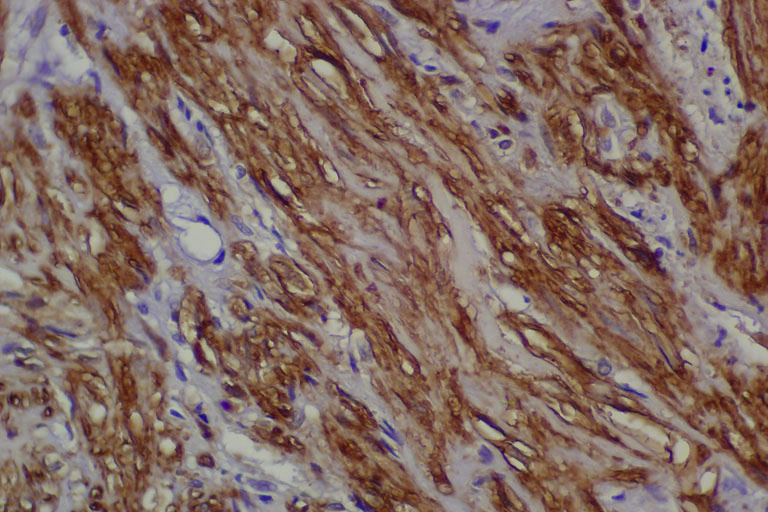
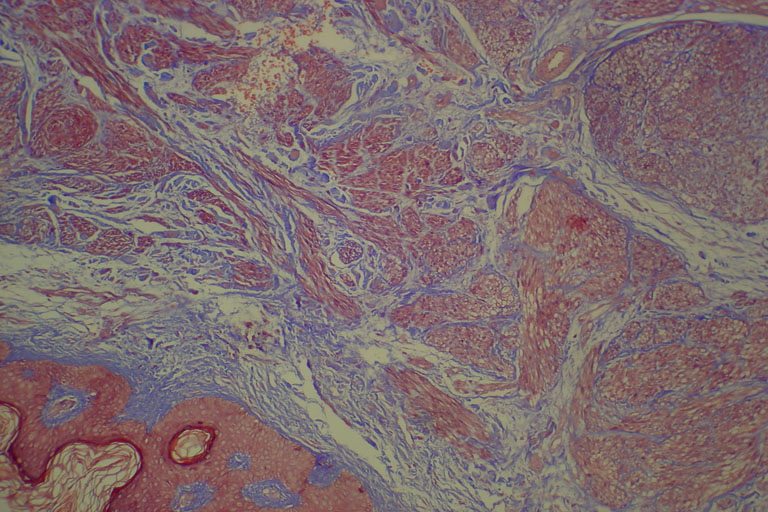
Microscopic examination showed a non-encapsulated mass in the dermis composed of spindle cells arranged in interlacing bundles with a vague fascicular pattern. There was no mitotic activity or atypical cells (Figure 2); necrosis was absent. The diagnosis was confirmed by immunohistochemical studies, which were positive for smooth muscle actin (Figure 3) and vimentin (Figure 4). In contrast, stains were negative for S100 protein (Figure 5). Masson’s trichrome stain revealed smooth muscle cells with bright red cytoplasm (Figure 6).
 |  |
| Figure 5 | Figure 6 |
|---|
Commentary
Leiomyoma was first described by Virchow in 1854 and it accounts for 3.8 percent of all benign soft tissue tumors [1].
Cutaneous leiomyomas are benign dermal tumors of smooth muscle. These uncommon tumors are categorized into the following three subsets: (1) solitary or multiple piloleiomyoma (from the erector pili muscles), (2) genital leiomyoma (from mammillary or genital muscle), and (3) angioleiomyoma (from muscle enveloping dermal blood vessels) [2].
There is controversy regarding the prevalence of solitary or multiple leiomyomas. In some reports multiple cutaneous leiomyomas are more common than solitary ones [3], but Heatley and Walsh have presented 28 solitary cutaneous leiomyomas diagnosed over a 10 year period; they have observed that solitary tumors are more common than multiple tumors [4].
Leiomyoma can occur at any age, but typically develop during adolescence or early adult life. Congenital leiomyoma is an extremely rare reported variant [5].
Montgomery and Winkelmann in 1958 reported a congenital case of axillary pilar leimyoma [6]. In another study, Lupton et al. reported a leiomyoma on an infant’s right heel present since birth [7].
In this article we report a case of solitary leiomyoma in an infant. There are few reports of solitary leiomyoma in the first year of life. Akay et al. have reported a two-month-old male infant with a solitary firm red nodule on his right cheek without any ulceration or necrosis [5]. Another report of infantile leiomyoma describes a congenital leiomyoma on the tongue presenting with airway obstruction [8]. In solitary forms, the extremities are mostly involved and in multiple leiomyoma, the trunk is affected more than the head and neck [5]. In Heatley’s study the tumor distribution was mainly on the extremities, but also occurred on the head and neck and genital skin [4].
In the precedent case reports, solitary lesions have been reported to measure up to 3 cm, but usually they are smaller than 2.6 cm [5].
The occipital localization of this tumor is an unusual site for cutaneous leiomyoma, which to our knowledge has never been reported.
References
1. Dassary BV, Khosraviani K, Irwin TS et al. Perianal Leiomyoma Involving the Anal sphincter. Ulster Med J 2007;76(3):173-174. [PubMed]2. Usmani N, Merchant W, Yung A . A case of cutaneous symplastic leiomyoma – a rare variant of cutaneous pilar leiomyoma. J Cutan Pathol 2008; 35(3):329-331. [PubMed]
3. Holst VA, Junkins-Hopkins JM, Elenitsas R. Cutaneous smooth muscle neoplasm: clinical features, histologic findings, and treatment options. J Am Acad Dermatol 2002;46:477-490. [PubMed]
4. Akay BN, Boyvat A, Heper AO et al. Congenital pilar leiomyoma, J Am Acad Dermatol 2008;59(5):102-104. [PubMed]
5. Berger TG, Levin MW. Congenital smooth muscle hamartoma. J Am Acad Dermatol 1984;11:709-712. [PubMed]
© 2010 Dermatology Online Journal