Cryotherapy as a treatment for psoriasis
Published Web Location
https://doi.org/10.5070/D3267351sgMain Content
Cryotherapy as a treatment for psoriasis
Sadollah Shamsadini, Majid Varesvazirian, and Ayeh Shamsadini
Dermatology Online Journal 11 (2): 21
Kerman university of Medical sciences Kerman Iran. shamsadini@yahoo.com
Abstract
There are very few publications on the use of cryotherapy in the treatment of psoriasis. We performed an evaluation to determine its efficacy in small plaque psoriasis. We selected 63 patients who had a clinical diagnosis of chronic plaque-type psoriasis and and for each patient we evaluated two psoriatic plaques of almost the same size and severity on similar areas of the body. One plaque was sprayed with liquid nitrogen every other day for two weeks and the other plaque was untreated as a control. Complete resolution of the plaque occurred in four patients (6.35 %), mild to moderate resolution was evident in 19 cases (30.1 %), and no improvement occurred in 40 patients (63.5 %). Only one complication, superimposed infection, occurred. Cryotherapy may mediates mild resolution of plaques by inducing normal re-epithelization following the physical destruction of the lesions via a reverse Koebner phenomenon. Our findings suggest that cryotherapy is safe to use in the treatment of small-plaque psoriasis but that its efficacy is limited.
Introduction
Cryotherapy is the application of intense cold to cause tissue necrosis by rapid freezing [1, 2]. The use of cryotherapy has been described for isolated localized small-plaque psoriasis [1]. The advantages of this treatment are that it is rapid, easy, safe, and produces little or no pain [3]. Use of this mode of treatment does not require an operating room, local anesthesia, sutures, dressings, or sterile techniques [4]. There currently are no drugs or methods of treatment that will safely induce permanent remission of psoriasis [5], therefore we undertook an evaluation of cryotherapy.
Methods
The study was conducted on 410 plaques of psoriasis (217 plaques in right side and 193 plaques in left side) of 63 outpatients (32 M and 31 F) with chronic plaque-type psoriasis who were attending the dermatology department, of Kerman University of Medical Sciences Faculty of Medicine, between 2001 and 2003. Mean age of our patients was 36 years and the ages ranged from 6 to 67. The plaque sizes were from 1.5 to 12 cm in diameter.
For each patient two psoriatic plaques of the same size and severity were selected on similar areas of the body. The patients were not using topical or systemic therapy for psoriasis and they were instructed not to treat the sites during the study period. The 217 plaques were sprayed every other day with liquid nitrogen for 2 weeks; the other 193 plaques were left untreated as a control group. The freezing time ranged from 9 to 15 seconds depending upon the size of the plaque. Routine topical antibiotic therapy (mupirocin cream) was applied after each session of cryotherapy for prophylaxis of infection on both groups. Patients were examined just before each session of cryotherapy to assess blister formation and response to treatment.
Results
|

|
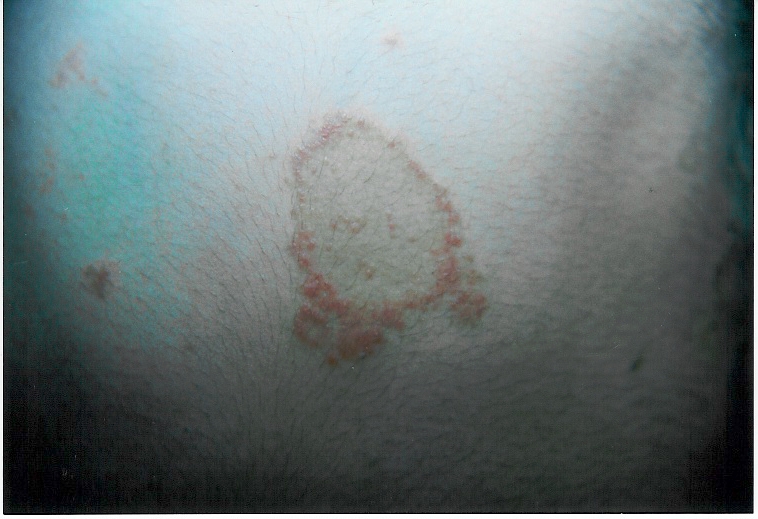
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Psoriatic plaque before treatment | |
| Figure 2. Following cryotherapy | |
All patients developed vesicles on the treated sites. Evidence of clinical improvement was made by assessment of erythema, induration, and scaling, and was graded as follows: 1-Complete resolution: absence of erythema, induration and scaling. 2- Moderate resolution: light pink, rare scale, slight elevation. 3- No resolution: very red, heavy scales, and marked ridge.
For the cryotherapy-treated sites, 4 patients (6.4% ) showed complete and 19 patients (30.1%) had mild to moderate resolution, and 40 other cases (63.5 %) had no resolution; On the untreated sites 3 cases (4.7 %) showed complete clearance, 18 cases (28.5 %) had mild to moderate resolution, and 42 cases (66/7%) were without improvement (Table 1). Generally the improvement after cryotherapy was better in older patients than younger and in patients with the larger lesion than smaller one (Tables 5).
Discussion
For 63 patients we evaluated the response of cryotherapy in 217 plaques of psoriasis on the right side compared to 193 untreated plaques on the left side. The results showed that cryotherapy can improve plaques of psoriasis a little more than in our control group.
Cryotherapy was first evaluated for psoriasis in 1987 by Scoggings who reported a response rate of 67-80 percent in 35 patients [6]. Later Nouri et al. treated nine patients with clinically diagnosed small-plaque psoriasis (plaque sizes 1-5 cm diameter) and obtained complete resolution in five patients (56 %), substantial resolution in two patients (2 %) mild resolution in one patient, and no resolution in the remaining patient [7]. Our patients had an improvement rate lower than those of Scoggings and Nouri [7, 8, 9].
In a study by Abd El Aziz on 50 patients with psoriasis, the response-no-response ratio was 6:1, far better than our patients [2].
Longer disease history and larger plaques were more often associated with a good response than better than shorter duration disease and smaller plaques. It seems likely that cryotherapy mediates mild resolution of plaques by inducing normal re-epithelization following the physical destruction of the lesions due to reverse Koebner phenomenon [10]. Our findings suggest that cryotherapy is safe to use in the treatment of small-plaque psoriasis but that its efficacy is limited.
References
1. Mark G Lebwohl. Psoriasis inverse psoriasis. Mark G Lebwohl Warren R Heymann John Bert-Jones and Ian Coulson.Treatment of skin Disease Mosby Harcourt Publishers Limited 2002 533-540.2. Abd El Aziz El-Taweel,M.D; Mohamed Kotb, M.D Ahmed Abd El Wahab,M. D; Adel Kamal, M.D. Adel Ali A;li M.D. Cryotherapy in Psoriasis. The Gulf journal of dermatology vol 6 Num 2 1999:46-8.
3. Chapin, M.E.; Burkes, E.L, and Hill, C.(1973): Cryosurgery of oral white lesion. J. Oral. Surg., 31:584-591.
4. Bassionny. A.; El-Meshad, M; Talaat, M.; kutty. K. and Metwaa, B. (1982): Cryosurgery in cutaneous leishmaniasis. Br. J. Dermatol., 107:467-474.
5. Hansen. J.E. (1971): Cryosurgery therapy of benign lesions of the skin and mucous membrane. Int. Surg. 56:402-406.
6. Fry, L. (1988): Psoriasis. Br. J. Dermatol. 119:445-461.
7. Scoggings, R.B. (1987): Cryotherapy for psoriasis. Br. J. Dermatol., 97:297.
8. Nouri, K.; Chartier, T.; Eaglstein, W.H. and Taylor, T.R. (1997): Cryortherapy for psoriasis Arch. Dermatol., 133: 1608-1609.
9. Stone. O.J. (1990): The elongated dermal papillae of psoriasis. Int. J. Dermatol., 29:187-189.
10. Eyre, R.E. W. and Krueger, G.G. (1982): Response to injury of skin involved and uninvolved with psoriasis and its relation to disease activity: Kobner and reveres kobner reaction. Br. J. Dermatol., 106:153-159.
© 2005 Dermatology Online Journal