Topical calcipotriol therapy in nail psoriasis :A study of 24 cases
Published Web Location
https://doi.org/10.5070/D31t20z9wwMain Content
Topical calcipotriol therapy in nail psoriasis :A study of 24 cases
Mehrnaz Zakeri Pharm D, Mahin Valikhani MD, Hossein Mortazavi MD, and Masoomeh Barzegari MD
Dermatology Online Journal 11 (3): 5
Department of Dermatology , Razi Dermatology Hospital,Tehran University of Medical Sciences,Tehran,Iran. zakerimehr@yahoo.com
Abstract
There are few reports regarding the treatment of nail psoriasis with topical calcipotriol. We undertook a case series study to evaluate the efficacy and safety of calcipotriol ointment (50 µg/g) in the treatment of nail psoriasis in 24 patients. This study involved 19 women and 5 men with nail psoriasis referred to Dermatology clinics of Razi hospital. The duration of trial was from October 2002 to September 2004. Informed consent was obtained from all patients before entering into the study. The patients applied calcipotriol ointment to the affected nails twice daily without occlusion for 3 months. Patients were seen by two academic dermatologists initially, after 2 weeks, and then at monthly intervals. The efficacy and safety were clinically assessed and any side effect was recorded. Patients who showed 50 percent or greater reduction in the baseline subungual thickness in at least one nail were considered to be responders and were offered continuation of therapy for an additional 2 months. After discontinuation of therapy, followup visits were performed at 1 and 2 months. After 3 months of therapy, fourteen patients showed significant clinical improvement, two of them were completely free from nail lesions after 5 months. Calcipotriol was particularly effective in subungual hyperkeratosis, onycholysis, and discoloration. In four patients fingertip tenderness and in one case the pain of involved distal phalanx were significantly reduced. No clinical response was observed in four patients. Only two cases showed adverse reactions. Topical Calcipotriol is an effective treatment for nail psoriasis and can be considered to be a safe topical treatment in chronic cases; its high tolerability allows prolonged usage without severe side effects.
Introduction
Nails are commonly involved in psoriasis with changes reported in 25-50 percent of psoriatic patients [1]. Characteristic nail changes in psoriasis include pitting, onycholysis, discoloration, subungual hyperkeratosis, nail dystrophy, and splinter hemorrhages [2].
In addition to cosmetic problems, nail psoriasis may cause some limitations in patient's daily activities. Nails in general are difficult to treat [3, 4, 5], respond slowly [3] and few therapeutic choices are satisfactory [6]. Topical treatments are barely effective and rarely induce complete remission of the disease, and possible side effects of systemic treatments limit their usefulness in uncomplicated nail psoriasis [7].
Calcipotriol, a structural analog of vitamin D3, is effective for local treatment of psoriasis vulgaris [5, 7, 8]. Few reports are available in the treatment of nail psoriasis with this drug [3, 7, 9]. In this study, we evaluated the efficacy and safety of calcipotriol ointment in the treatment of nail psoriasis.
Patients and methods
Nineteen women and five men with nail psoriasis referred to Dermatology clinics of Razi hospital entered the study. The duration of trial was from October 2002 to September 2004. Eligible patients were over 18 years of age, of either sex, with clinical diagnosis of nail psoriasis (including pitting, onycholysis, discoloration, subungual hyperkeratosis, and nail deformity) [1, 4, 5]. Direct microscopy and cultures were performed to rule out onychomycosis. Pregnant or breast-feeding women were excluded, as were patients with severe hepatic insufficiency, those who had received vitamin D based therapies, or topical or systemic treatments of psoriasis in past 2 months. Informed consent was obtained from all patients before entering into the study.
In this study 24 patients aged 18-68 years (mean age 33) received topical calcipotriol. The duration of nail involvement ranged between 1 month and 14 years. In fifteen patients both fingernails and toenails were involved, and nine cases had only fingernail involvement. All patients showed subungual hyperkeratosis (>1mm for fingernails, >2.5mm for toenails) and onycholysis. Pitting was present in sixteen, and nail deformity in nine cases (Table 1). Twenty patients had previously taken other therapies as topical or intralesional steroids, topical methoxsalen and 5-fluorouracil.
Patients were instructed to apply calcipotriol ointment (50 µg/g) without occlusion twice daily to the affected nail plates, lateral and proximal nail folds. The patients were seen initially, after 2 weeks, and then monthly. Followup visits were performed by two academic dermatologists. The efficacy and safety were clinically assessed and any side effect was recorded. The duration of treatment was 3 months. Patients who showed 50 percent or greater reduction in the baseline hyperkeratotic thickness at least in one nail, were considered as responders and offered continuation of therapy for an additional 2 months. Followup visits were performed at one and 2 months after discontinuation of therapy.
Results
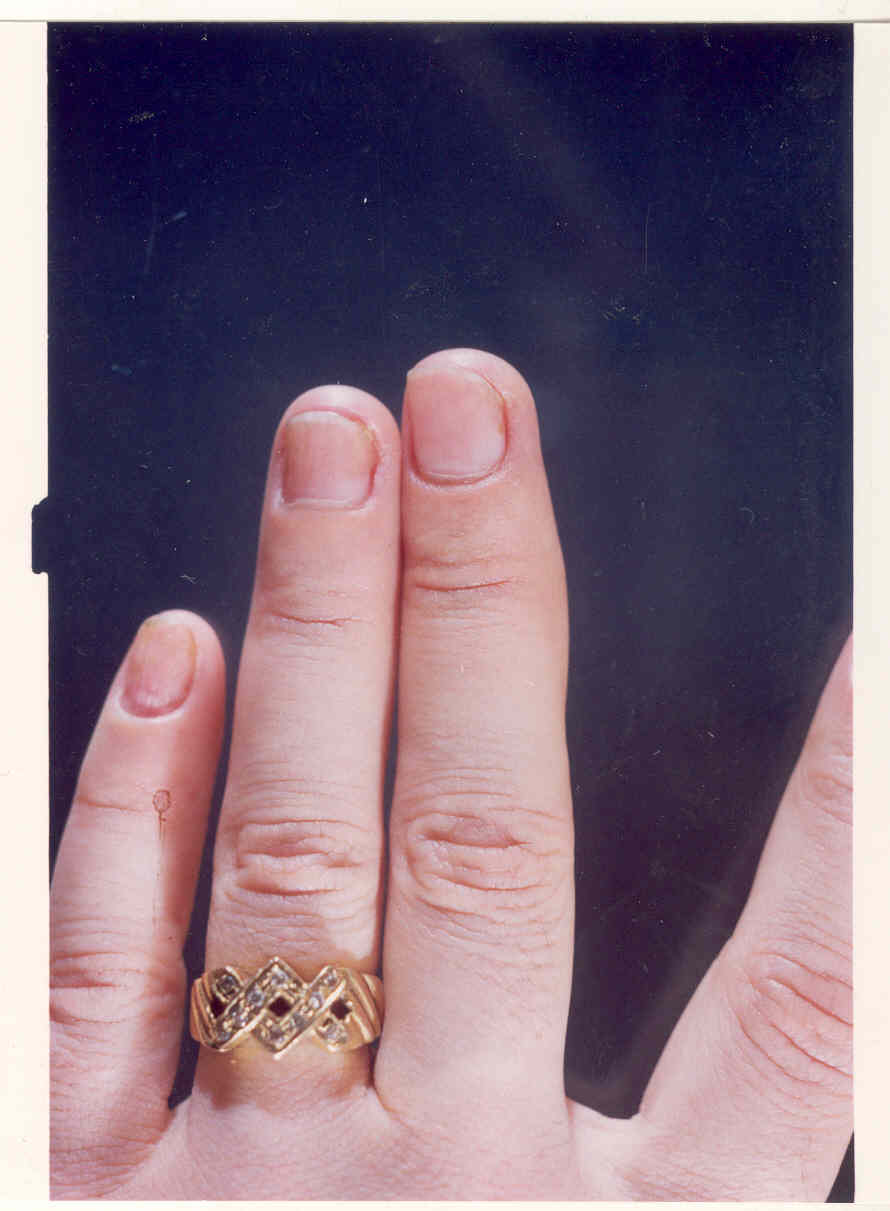
After 3 months of therapy, fourteen patients showed significant improvement; two were completely free from nail lesions after 5 months. Calcipotriol was particularly effective in reducing hyperkeratosis, onycholysis, and discoloration (Figs. 1A and 1B). Fingernails responded better than toenails. In four patients fingertip tenderness was significantly reduced parallel to improving clinical signs; and in one patient the pain of involved distal phalanx was reduced despite the persistence of nail lesions. No clinical response was observed in four patients. They had been previously treated with topical and /or intralesional steroids without any success. Adverse reactions were seen in two patients (periungual irritation and inflammation in one, irritation, pruritus and oozing in the other). These patients withdrawn from the study. Four patients were lost to followup and were considered drop outs. After discontinuation of therapy, the majority of patients experienced recurrent lesions with much lower severity.

|
|
| Figure 1a | Figure 1b |
|---|---|
| Fig. 1A. Fingernails of a 27 year-old woman before starting treatment . | |
| Fig. 1B. Same patient after 5 months of topical calcipotriol treatment . | |
Discussion
Psoriasis is frequently accompanied by nail changes that, in some cases, produce severe functional limitations. Treatment of nail psoriasis is difficult [2, 4 5]. Systemic agents such as methotrexate [4, 5, 8] Acitretin , etretinate [8, 10], and cyclosporin [5, 8] are useful but seldom justified for nail disease alone [4, 5]. PUVA or topical application and intralesional injection of corticosteroids and PUVA may be effective but are not usually practical or highly effective [4]. Topical 5-fluorouracil is reported to be effective in subungual hyperkeratosis and pitting, but it is contraindicated in onycholysis [8].
Topical cyclosporin has also been used successfully in one patient [8]. Calcipotriol is a synthetic analog of vitamin D3 that inhibits keratinocyte proliferation and induces terminal differentiation [5, 8, 11]. Calcipotriol is effective for psoriasis [5, 8, 11], and a few studies report efficacy in nail psoriasis [3, 7, 9]. This study shows the efficacy of calcipotriol in 24 patients with nail psoriasis. In this study fourteen patients showed significant clinical improvement after 3 months of therapy, and two of them became completely lesion-free after another 2 months. In a report by Kokelj et al. five of seven patients showed subjective and objective improvement after 3 months of calcipotriol cream application, and one of the responders showed complete clearance of nail lesions after another 3 months of treatment [7].
Our study indicates that fingernails respond better than toenails, confirming a previous study [9]. This may be due to the more severe hyperkeratosis of toenails, their slower growth rate, poorer penetration of the calcipotriol, or perhaps differences in compliance with treatment.
This was an open study; clearly the lack of a control group limits the evaluation of calcipotriol for nail psoriasis. To obtain more strong evidence for the benefits of calcipotriol on nail psoriasis, controlled trials especially randomized clinical trials are suggested to be performed and further research in this area is needed.
Conclusions
Topical calcipotriol is an effective treatment for nail psoriasis, its high tolerability allows its prolonged usage without severe side effects. Therefore it can be considered to be a safe topical treatment in chronic cases.
Aknowledgment :We would like to thank Dr. M Danesh-Pajooh for her kind contribution in this study.
The calcipotriol (Daivonex®) that our patients used is the product of LEO pharmaceutical company.
References
1. Camp RDR. Psoriasis . In: Textbook of Dermatol , 6th Edition , vol 2. oxford : Blackwell Science , 1998 : 16032. De. Jong EMGJ, Seegers BAMPA , Gulinck MK. Psoriasis of the nails associated with dlsability in a large number of patients : Results of a recent interview with 1,728 patients. Dermatol. 1996;193:300 - 303
3. Petrow W. Treatment of a nail psoriasis with topical calcipotriol . Aktuel Dermatol. 1995; 21 : 396 - 400
4. Robert S,Stern and Jessica WU. Psoriasis . In : Arndt KA , leboit PE, Robinson JK, Wintroub BU. Cutaneous medicine and surgery , Vol 1.Philadelphia : W.B. Saunders , 1996; 316
5. Baran R , Tosti A. Nails . In : Fitzpatric TB, Eisen AZ, Wolff K. Dematol in general medicine , 5th edition , vol 1. New york: Mc Graw - Hill , 1999; 757-8
6. Yamamoto T , Katayama I, Nishioka K. Topical anthralin therapy for refractory nail psoriasis . J Dermatol. 1998; 25 :231 -3
7. Kokelj F , Lavaroni G, Piraccini BM. Nail psoriasis treated with calcipotriol ( MC 903 ): An open study . J Dermatol Treat. 1994; 5: 149-50
8. Dawber RPR , Baran R,BERker D.Disoders of nails . In : Champion RH, Burton JL, Burns DA, Breathnach SM.Textbook of Dermatol , 6th edition, Vol 4. Oxford : Black well Science , 1998; 2839- 41
9. Tosti A, piracini BM, Cameli N. calcipotriol onitment in nail psoriasis : a controlled double-blind comparison with betamethason dipropionate and salicylic acid . British J Dermatol. 1998; 139 : 655-9
10. Zouboulis CC, orfanos CE. Retinoids . In : Millikan LE. Drug therapy in Dermatol. Marcel Dekker Inc , 2000; 189 - 192
11. Murdoch D, Clissod sp. Calcipotriol . A review of its pharmacological properties and therapeutic use in psoriasis vulgaris . Drugs. 1992; 43 : 415 - 29
© 2005 Dermatology Online Journal