Linear porokeratosis
Published Web Location
https://doi.org/10.5070/D31k91q36rMain Content
Linear porokeratosis
SK Malhotra, KJPS Puri, Tanu Goyal, KS Chahal
Dermatology Online Journal 13 (4): 15
Government Medical College, Amritsar, IndiaAbstract
Linear porokeratosis is a rare variant. It can be present at birth or can develop in adult life. Lesions of linear porokeratosis are grouped and linearly arranged along the lines of Blaschko. On the extremities it affects the distal portion more than the proximal areas. On the trunk these can be zosteriform in distribution. Lesions of linear porokeratosis probably result from an abnormal clone of epidermal precursors. A 20 year old male presented with annular plaques in linear pattern following the lines of Blaschko over the left upper limb extending up to the axilla present since childhood. The lesions had atrophic centre and raised hyperkeratotic borders. The lesions were more proximal than distal. Few scattered lesions were present on left side of trunk. There was no family history of such lesions. Systemic examination of patient was normal. On histopathological examination there was hyperkeratosis and parakeratosis. A coronoid lamella was present. At the base of coronoid lamella thinned out granular layer and necrotic keratinocytes were also seen. In the dermis pigment incontinence and perivascular lymphocytic infiltrate were present. This case is being reported because of its rarity. It is an atypical presentation because the lesions were disposed more over proximal than distal area of upper limb. Linear porokeratosis is associated with an increased risk of malignant transformation.
Porokeratosis is a disorder of keratinization characterized clinically by sharply demarcated, hyperkeratotic, annular lesions with distinct keratotic edge corresponding histologically to the presence of coronoid lamella, a column of parakeratotic cells extending through the stratum corneum. Five clinical variants of porokeratosis have been recognized as follows: 1) classic porokeratosis of mibelli (PM); 2) disseminated superficial porokeratosis (DSP) and disseminated superficial actinic porokeratosis (DSAP); 3) porokeratosis palmaris et plantaris disseminata (PPPD); 4) linear porokeratosis; and 5) punctate porokeratosis.
The etiology of various types of porokeratosis is unknown. An autosomal dominant mode of inheritance has been reasonably well established for PM [1, 2], PPPD [3], DSP and DSAP[4]. We report a case of linear porokeratosis involving the left upper limb.
Clinical synopsis
A 20-year-old man presented in the Dermatology OPD of Government Medical College Amritsar (India) with annular plaques in a linear array over the left upper limb present since childhood. There was no family history of similar lesions. General physical examination and systemic examination of the patient was normal. Cutaneous examination revealed the presence of multiple discrete and grouped annular plaques presenting linearly along the lines of Blaschko on the left upper limb extending into the axilla (Fig. 1).
 |  |
| Figure 1 | Figure 1 |
|---|
The lesions had atrophic centers with raised hyperkeratotic borders (Fig. 2). They was more involvement of the proximal area than of the distal area of limb. Few scattered lesions were present over left side of abdomen and back.
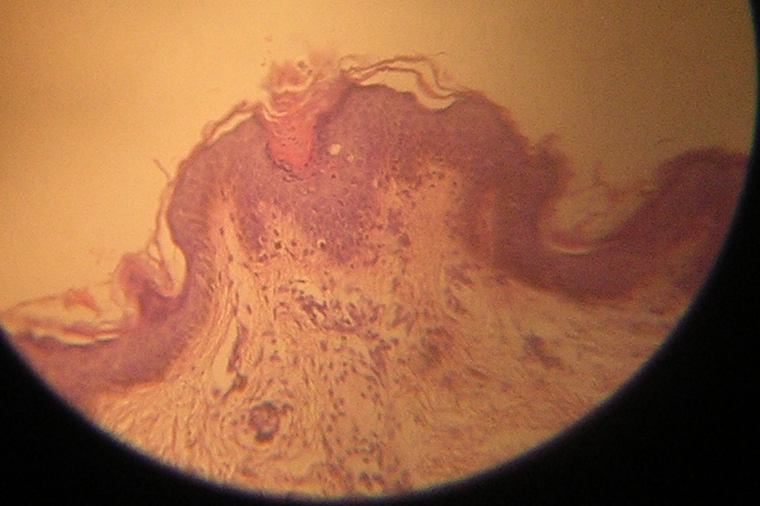 |
| Figure 3 |
|---|
Hematological (Hb, TLC, DLC, PBF) and biochemical (SGOT, SGPT, blood urea, Serum creatinine, FBS) investigations were within normal limits. On histopathological examination, there was hyperkeratosis and papillomatosis. A coronoid lamella was present overlying a thinned granular layer. Necrotic keratinocytes were also present. In the dermis pigment incontinence and perivascular lymphohistiocytic infiltrate was also present (Fig. 3).
The clinical and histologic findings were consistent with the diagnosis of porokeratosis.
Discussion
Linear porokeratosis is listed as a rare disease by Office of Rare Diseases (ORD) of the National Institute of Health, meaning thereby that linear porokeratosis affects fewer than 20,000 people in the US population. It occurs in a unilateral, linear form resembling linear verrucous epidermal nevus [5]. Linear porokeratosis following lines of Blaschko can present at birth or may not develop until adult life. Occasionally, there is family history of linear porokeratosis or other kind of porokeratosis such as disseminated superficial actinic porokeratosis, suggesting genetic predisposition. Linear porokeratosis has been observed in monozygotic twins [6]. The lesions of linear porokeratosis are grouped and linearly arranged on extremities affecting the distal portion more than the proximal areas and on the trunk they may be present in zosteriform distribution [7]. In our case, lesions were present since childhood and were distributed more over proximal than distal areas of limb.
The lesions of porokeratosis probably result from an abnormal clone of epidermal precursors. Malignant degeneration and metastasis are reported for this variety [8, 9], which can be either basal cell carcinoma or squamous cell carcinoma and most likely occur in older adults. A genetic mechanism of allelic loss may represent an initial step in the development of cancer [10]. The development of a nodule or sore within a porokeratosis lesion warrants biopsy evaluation. Other medical conditions reported in association with porokeratosis include immunosuppression, being a recipient of organ transplantation, burn scar, Crohn disease, and liver disease [11, 12, 13, 14]. None of these conditions were present in our case.
References
1. Gilchrest TC. Eleven cases of porokeratosis (Mibelli) in one family. J Cutaneous Genitourin Dis 1899; 17: 149.2. Sehgal VN, Dube B. Porokeratosis (Mibelli) in a family. Dermatological 1967; 134: 219.
3. Guss SB et al. Porokeratosis plantaris, palmaris et disseminata: A third type of porokeratosis. Arch Dermatol 1971; 104: 366.
4. Anderson DE, Chernosky MF. Diseminated superficial actinic porokeratosis. Genetic aspects. Arch Dermatol 99: 408, 1969.
5. Truffi M. Sur un cas de porokeratosis systemisee. Ann Dermatol Syphiligr 1905; 6: 521.
6. Guillot P et al. Porokeratosis de Mibelli lineaire chez des Jumelles monozygotes. Ann Dermatol Venereol 1991; 118: 519.
7. Goldner RM. Zosteriform porokeratosis of Mibelli: Arch Dermatol 1971; 104: 425.
8. Friedman SJ. Herman PS, Pittelkow MR. Punctate Porokeratosis keratoderma. Arch Dermatol 1988; 124: 1678-82.
9. Lozinski AZ, Fisher BK, Walter JB et al. Metastatic squamous cell carcinoma in linear porokeratosis of Mibelli J Am Acad Dermatol 1987; 16: 448-51.
10. Happle R. Cancer Proneness of linear porokeratosis may be explained by allelic loss. Dermatology 1997; 195(1): 20-25.
11. Kanitakis J et al. Porokeratosis in organ transplant recipient. J Am Acad Dermatol 2001;44:144.
12. Nova MP et al.Porokeratosis arising in burn scar1991;25:354.
13. Morton CA et al. Porokeratosia and Crohn’s disease. . J Am Acad Dermatol 1995;32:894.
14. Hunt SJ et al. Linear and punctuate porokeratosis associated with end stage liver disease.J Am Acad Dermatol 1991;25:937.
© 2007 Dermatology Online Journal