Isolated annular lichen planus of lower lip
Published Web Location
https://doi.org/10.5070/D31jm3n2ggMain Content
Letter: Isolated annular lichen planus of lower lip
Sarika Holmukhe DNB, Rameshwar Madhukarrao Gutte MD, Subodh Sirur MD
Dermatology Online Journal 18 (2): 15
MGM Hospital and ESIC-PGIMSR, Parel, Mumbai-12, IndiaAbstract
Lichen planus (LP), the prototype of lichenoid dermatoses, is an idiopathic inflammatory disease of the skin and mucous membranes, hair follicles, and nails. It rarely occurs on the lips and usually then in association with oral lesions. We report a 40-year-old man with a 3-month history of an isolated single annular violaceous plaque of the lower lip. The rest of his mucosae, skin, hair and nails were normal. Histopathology confirmed the diagnosis of LP. The patient was advised to use topical tacrolimus 0.03 percent cream twice daily along with multivitamins, but the patient was lost to follow-up. Isolated LP of the lip is unusual, although this condition may be underestimated and therefore under-reported in the literature [1].
Introduction
The term LP was first introduced in 1869 by Erasmus Wilson, thereby renaming a condition that had been described by Hebra as lichen ruber [2]. The disease is thought to affect approximately 0.5 percent to 1 percent of the population worldwide [3].
Oral LP occurs most often on the buccal mucosa, but the gingivae, tongue, floor of the mouth, retromalar pads and lips may also be affected [4]. Lip localization has an increased risk, because external trauma, smoking, and ultraviolet light trigger malignant transformation. Only a few cases of isolated LP of the lips have been reported until now [5]. Most commonly it presents as mucosal erosions, although rarely other morphologies like bullous lesions have been described [6].
Herein, we report a case of isolated lower lip LP presenting as a solitary annular lesion.
Case report
 |
| Figure 1 |
|---|
| Figure 1. A solitary annular violaceous plaque on the lower lip with raised margin. |
A 40-year-old married male presented to us with an asymptomatic solitary violaceous raised annular lesion over right angle of the lower lip for 3 months. There was no history of similar complaints in the past or family history of similar complaints. There was neither history of any topical application prior to development of the lesion or after it.
Cutaneous examination revealed a solitary annular violaceous plaque of 1 cm x 1.5 cm size with a raised margin over lower lip (Figure 1). The outer edge was raised with a somewhat beaded appearance, whereas the inner edge was macerated. The rest of the cutaneous and systemic examination was within normal limits.
A differential diagnosis of discoid lupus erythematosus, mucosal LP, mucosal porokeratosis, and superficial spreading basal cell carcinoma (BCC) were considered.
On investigations, complete blood count with differential liver and kidney function tests, and urine and stool microscopy showed no abnormality. No serological evidence of hepatitis C virus (HCV) infection was found.
 |  |
| Figure 2 | Figure 3 |
|---|---|
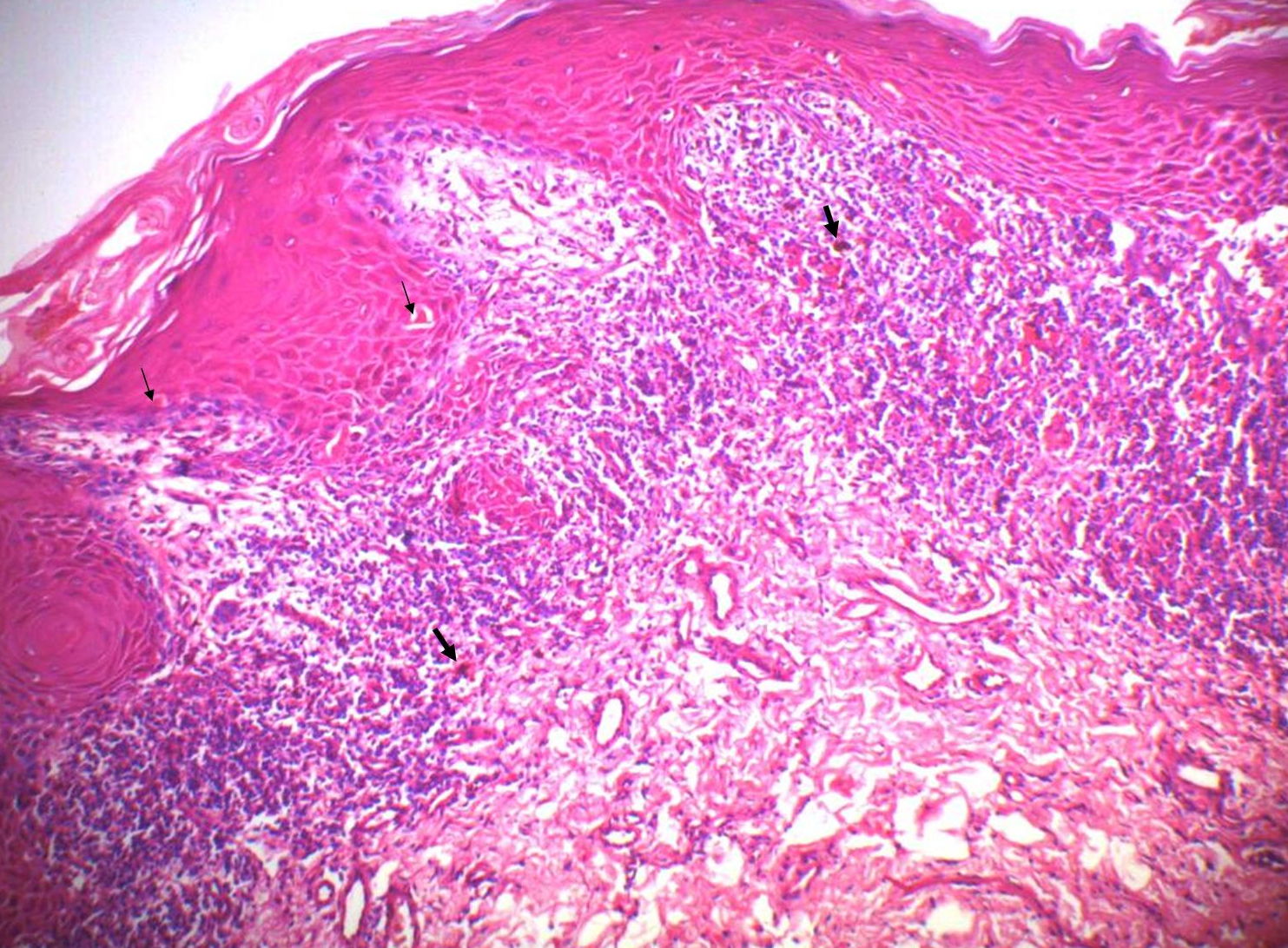
| Figure 2. A scanning view of biopsy from lesion showing irregular epidermal hyperplasia, band-like infiltrate, interface changes,
and dermal melanophages. (H&E, x50) Figure 3. High power view showing irregular epidermal hyperplasia, lichenoid infiltrate of lymphocytes, necrotic keratinocytes (Small arrows) and melanophages (Large arrows) with squamatization of the basal layer. (H&E, x200) | |
A 3 mm biopsy from the edge of the plaque showed classic features of LP, including a band-like lymphocytic infiltrate, interface vacuolar changes, necrotic keratinocytes, and dermal melanophages. No atypical keratinocytes or solar elastosis was seen. Based on the clinico-pathological correlation, a diagnosis of isolated annular LP of the lip was made.
The patient was advised to start topical tacrolimus 0.03 percent cream twice daily along with multivitamins, but the patient was lost to follow-up. This report describes LP exclusively localized on the lower lip with the rare morphologic presentation of a solitary annular plaque.
Discussion
The isolated occurrence of LP on the lip has been well documented in only a few reports. In most of the cases there was diffuse involvement of the lower lip along its entire length [1].
The first well documented case of isolated lip LP was reported by P. H. Itin et al. The patient presented with erosive lesions with swelling and crusting, which resolved completely with oral acitretin and prednisone [4]. Another case showed irregular white streaks in a reticular pattern, which healed with betamethasone valerate 0.1 percent cream [7]. A third case of 11 years duration in a 52-year-old woman with LP of the vermilion border and skin of the lower lip, successfully treated with chloroquine phosphate was reported [8]. R. Cecchi and A. Giomi in 2002, reported a probable fourth case of isolated lip LP treated successfully with topical betamethasone dipropionate 0.5 percent ointment. However, four months later, the patient developed typical cutaneous LP [1]. A case of a 44-year-old man who presented with a 3-year history of isolated lower lip erosions, for which the diagnosis of LP was made, was reported by in 2003 by Yu TC et al. [9].
M. Petruzzi et al. in 2007 reported a case series of 10 patients with isolated lip LP. The atrophic-erosive form was the most common in their series and five cases had HCV hepatitis. A complete remission of lesions was observed in eight patients after topical treatment with clobetasol propionate 0.05 percent and tocopherol oil, whereas partial improvement was noted in those remaining [10]. Another series of four cases of isolated lip LP was reported by G. Gencoglan et al. They successfully treated 3 cases with imiquimod 5 percent cream, applied twice daily, 5 days a week, for 2 weeks. Only one recurrence was observed during the 5, 10, and 18 months' follow-up period [5]. Results of these larger series of isolated lip LP suggest that it might be underestimated.
According to Andreasen, oral LP can be classified into six types: reticular, papular, plaque-like, erosive, atrophic, and bullous [11]. Our case, showed an annular plaque with raised margin and slight atrophy at the center. This peculiar morphologic presentation creates a vast number of clinical differential diagnoses. For example, the differential diagnosis of bullous LP includes LP pemphigoides, bullous pemphigoid, pemphigus vulgaris, erythema multiforme, and herpes simplex virus infection [6]. Moreover, the presence of a raised margin with beaded appearance in our case, lead us to think of porokeratosis and BCC.
Different regimens for the treatment of oral LP have been reported, including corticosteroids (topical, intralesional, and systemic), topical and oral retinoids, griseofulvin, azathioprine, mycophenolate, dapsone, cyclosporin, imiquimod 5 percent cream, tacrolimus, and choloroquine phosphate [1, 5, 6, 8, 10].
Chronic inflammation coupled with exposure to various carcinogens like smoking, ultraviolet radiation, alcohol, poor nutrition, and poor dentition causing repeated trauma poses a risk of malignant transformation in lip LP. A case of sqaumous cell carcinoma complicating lip LP in a 23-year-old patient has been documented [12].
Close observation and active early treatment are necessary to improve symptoms and might also be a relevant prevention strategy for squamous cell carcinoma risk [10].
In conclusion our case represents one of the rare presentations of LP with isolated lip involvement and the rare morphology of an annular plaque with raised margin.
References
1. Cecchi, R. and Giomi A. Isolated lichen planus of the lip. Aus J Dermatol, 2002; 43: 309-310 [PubMed].2. Wilson E. On lichen planus. J Cutan Med Dis Skin 1869; 3: 117-132.
3. Mollaoglu N. Oral lichen planus: a review. Br J Oral Max Surg 2000; 38: 370-377.
4. Itin PH, Schiller P, Gilli L, Buechner SA. Isolated lichen planus of the lip. Br J Dermatol. 1995;132(6):1000-2 [PubMed].
5. Gencoglan G, İnanir İ, Sahin O, Gunduz K. Imiquimod 5% cream for isolated lichen planus of the lip. J Dermatolog Treat. 2011;22(1):55-9 [PubMed].
6. Van Tuyll van Serooskerken AM, Van Marion AMW, De Zwart-Storm E, Frank J, Poblete-Gutiérrez P. Lichen planus with bullous manifestation on the lip. Int J Dermatol 2007; 46: 25-26 [PubMed].
7. Allan SJR, Buxton PK. Isolated lichen planus of the lip. Br. J. Dermatol. 1996; 135: 145-6 [PubMed].
8. De Argila D, Gonzalo A, Pimentel J, Rovira I. Isolated lichen planus of the lip successfully treated with chloroquine phosphate. Dermatology 1997;195(3):284-5 [PubMed].
9. Yu TC, Kelly SC, Weinberg JM, Scheinfeld NS. Isolated lichen planus of the lower lip. Cutis. 2003 Mar;71(3):210-2 [PubMed].
10. Petruzzi M, De Benedittis M, Pastore L, Pannone G, Grassi FR, Serpico R. Isolated lichen planus of the lip. Int J Immunopathol Pharmacol. 2007 Jul-Sep; 20(3):631-5 [PubMed].
11. Andreasen JO. Oral lichen planus. A clinical evaluation of 115 cases. Oral Surg Oral Med Oral Pathol 1968; 25: 31-42 [PubMed].
12. Harland CC, Phipps AR, Marsden RA, Holden CA Squamous cell carcinoma complicating lichen planus of the lip. J R Soc Med. 1992 Apr;85(4):235-6 [PubMed].
© 2012 Dermatology Online Journal