Contact reaction associated with Techni-care® Surgical Scrub
Published Web Location
https://doi.org/10.5070/D31ff7f9vpMain Content
Contact reaction associated with Techni-care® Surgical Scrub
Cara Freeland MD1, Ravi S Krishnan MD2, Heidi B Donnelly MD 3
Dermatology Online Journal 15 (2): 14
1. Department of Dermatology, Indiana University School of Medicine, Indianapolis, Indiana2. Director of Dermatologic Surgery, Assistant Professor, Department of Dermatology, Indiana University School of Medicine, Indianapolis, Indiana. ravi.krishnan@gmail.com
3. Dayton Skin Surgery Center, Dayton, Ohio
Case report
 |
| Figure 1 |
|---|
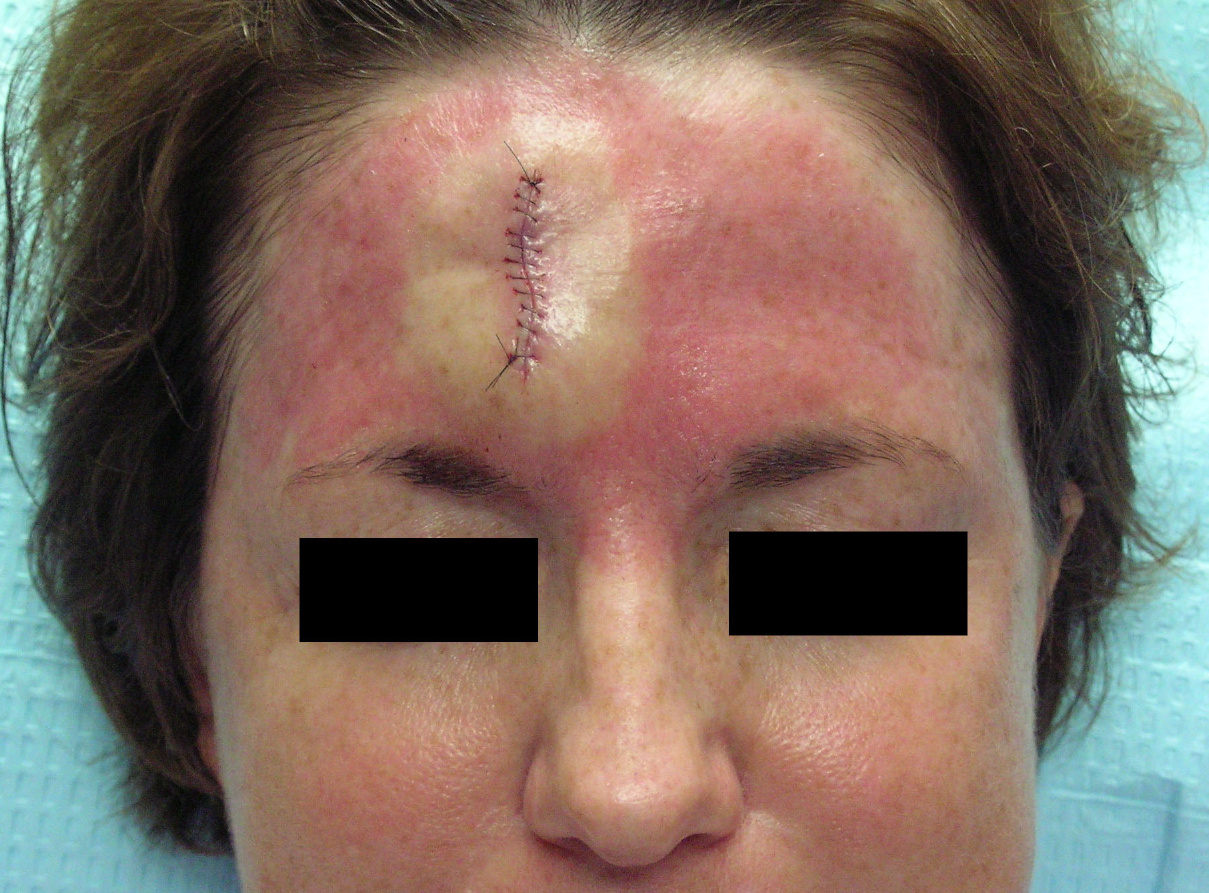
| Figure 1. Appearance of patient's forehead 15 minutes after Techni-care surgical scrub was applied. The blanched area was anesthetized with 1 percent lidocaine with 1:100000 epinephrine prior to application of the Techni-care. |
Our patient is a 46-year-old, white female who was referred to our office for the treatment of a basal cell carcinoma on her forehead. She underwent a two-stage Mohs procedure to remove the tumor, followed by a primary closure to repair the surgical defect. Prior to each stage, the tumor and the surrounding skin were cleansed with Techni-care surgical scrub. Prior to the reconstruction, the patient's entire forehead, brows, and glabella were cleansed with the Techni-care. After the reconstruction, which took approximately 15 minutes, the patient was observed to have a diffuse erythematous patch across her forehead (Fig. 1). The area immediately adjacent to the surgical site, which had been infiltrated with 1 percent lidocaine with 1:100,000 epinephrine, was blanched. The patient stated that she had noticed some mild pruritus near the surgical site throughout the day and that it was more significant after the reconstruction. The patient was given some desonide cream to apply to the area. When she returned for suture removal the following week, she reported that the rash had completely resolved after one day. She also mentioned that she had only applied the desonide cream once. The patient returned about two months later for follow-up, at which time she said that she had no further recurrence of the rash. She denied ever having had a similar rash either before or after surgery. We offered the patient patch testing or a reapplication test to further elucidate the etiology of her eruption, but she declined.
Discussion
Our patient developed a rash within one hour of applying Techni-care surgical scrub that completely resolved within one day. We have used Techni-care in over 3,000 cases without encountering any adverse reactions to the surgical scrub. Techni-care is a widely used surgical scrub, which, according to studies performed by the manufacturer, eliminates 99 percent of gram positive and gram negative bacteria in 30 seconds [1]. Other studies have also found it to be an effective anti-microbial agent [2]. In addition, after performing a literature search and contacting Techni-care's manufacturer, Care-tech, we have not found any known reports of contact dermatitis since the product's release in February 1991.
The differential diagnosis for the contact dermatitis that developed in our patient is allergic contact dermatitis (ACD), irritant contact dermatitis (ICD), and contact urticaria. Because of the timeframe of the reaction, it is unlikely to be ACD. ACD is a delayed hypersensitivity immune reaction that does not normally occur until 24-48 hours after application of the allergen [3]. In contrast, ICD may develop in minutes or hours but typically takes longer than a day or even weeks to completely resolve, depending on the damage to the skin. However, in contact urticaria, the reaction normally appears within an hour and resolves completely within a few hours, leaving no evidence of irritation [4]. While contact urticaria normally produces a raised wheal – not seen in our patient – it still possible to observe urticarial lesions that are macular. Given the rapid onset and resolution of the patient's eruption, she most likely experienced either an irritant contact dermatitis or a contact urticaria.
Techni-care is composed of 3 percent chloroxylenol, which is the active ingredient, and other inactive ingredients, including aloe vera gel, citric acid, cocamidopropyl betane, cocamide DEA, cocamidopropyl PG-dimonium chloride phosphate, D&C Yellow #1, hydrolyzed collagen, propylene glycol, sodium lauryl sulfate, tetrasodium EDTA, and water.
Choroxylenol, the active ingredient, is a chlorinated phenol antiseptic that is found in many over-the-counter products, especially liquid soaps used in industrial and health care environments. Chloroxylenol has only been known to cause ACD with a 1.4 percent sensitivity rate according to the North American Contact Dermatitis Group [5]. Despite its relationship with ACD, there have been no known reports of contact urticaria.
For the inactive ingredients, sodium lauryl sulfate (SLS), aloe vera, hydrolyzed collagen, and propylene glycol have rarely been reported to cause contact uriticaria. Sodium lauryl sulfate is a known irritant, but in certain circumstances, it is reported that SLS can likely provoke non-immunogenic contact urticaria due to the chronology, dose effect, and histology of some of the reactions. However, these cases occurred in animal models [6].
Morrow et al. report a case of contact urticaria to aloe leaf jelly, but this was not purified aloe gel (aloe pulp) [7]. However, in a more recent series, Reider et al. explain that all previous reactions with aloe were from the unprocessed aloe leaf which contained anthrachinone leaf extracts. They conclude that the sensitizing capacity of aloe vera gel, which is now in most products, appears to be very low [8].
Hydrolyzed collagen, a protein hydrolysate used in hair conditioners, is reported to cause contact urticaria. However, the study found that most subjects that developed the contact urticaria had atopic dermatitis and reacted to hydroxypropyl trimonium hydrolyzed collagen, which has a higher average molecular weight than hydrolyzed collagen [9].
Propylene glycol has been shown to be a mild irritant, an allergen in a small percentage of cases, and according to Funk and Maibach, it can cause non-immunologic contact urticaria after being topically applied to the skin [10], so it would seem to be the most likely cause of our patient's contact urticaria. However, there are some features of her presentation which are not consistent with this hypothesis. Since propylene glycol is a solvent and humectant that is widely used in cosmetics, foods, and pharmaceuticals, it seems odd that she never experienced a prior contact urticaria to products containing propylene glycol. Moreover, after thoroughly questioning the patient, we learned that since the resolution of her contact urticaria, the patient has used several products containing propylene glycol without any reactions.
While the specific component of the Techni-care that caused our patient's reaction is not entirely certain, it is reassuring to note that the eruption resolved without sequelae rather rapidly. Since Techni-care is a commonly used surgical scrub, it is important that those who use it are aware of this potential side-effect. Given the frequency with which we use Techni-care in our clinics (it is used prior to taking all Mohs layers and prior to all reconstructions), we can confidently say that this type of reaction is a fairly uncommon one. Furthermore, if it is encountered, while the eruption itself is quite striking, the patient can be reassured that it will probably resolve quickly.
References
1. Delasco. Techni-Care® Surgical Scrub. Available at: http://www.delasco.com/pcat/1/Protection/TC12/TC12/(Accessed: February 4, 2008)
2. Grubbs BC, Statz CL, Johnson EM, Uknis ME, Lee JT, Dunn DL. Salvage Therapy of Open, Infected Surgical Wounds: A Retrospective Review Using Techni-Care®. Surgical Infections 2000; 1: 109-114. [PubMed]
3. Mark BJ, Slavin RG. Allergic Contact Dermatitis. Med Clin North Am. 2006; 1: 169-85. [PubMed]
4. Wakelin S. Contact urticaria. Clinical and experimental dermatology 2001; 26:132-136. [PubMed]
5. Mowad C. Chloroxylenol causing hand dermatitis in a plumber. Am J Contact Dermat 1998; 9:128-129. [PubMed]
6. Anderson C. Irritant contact reactions versus non-immunologic contact urticaria. Acta Derm Venereol 1988; 68 suppl 135:45-48. [PubMed]
7. Morrow D, Rapaport M, and Strick R. Hypersensitivity to aloe. Arch Dermatol 1980; 116:1064-1064. [PubMed]
8. Reider N, Issa A, Hawranek T, Schuster C, Aberer W et al. Absence of contact sensitization to aloe vera. Contact Dermatitis 2005; 53: 332-334. [PubMed]
9. Niinimaki A, Niinimaki M, Makinen-Kiljunen S, Hannuksela M. Contact urticaria from protein hydrolysates in hair conditioners. Allergy 1998; 53: 1078-1081. [PubMed]
10. Funk J, Maibach H. Propylene glycol dermatitis: re-evaluation of an old problem. Contact Dermatitis 1994; 31:236-241. [PubMed]
© 2009 Dermatology Online Journal