Oral and cutaneous lichenoid reaction with nail changes secondary to imatinib: Report of a case and literature review
Published Web Location
https://doi.org/10.5070/D319t833jhMain Content
Oral and cutaneous lichenoid reaction with nail changes secondary to imatinib: report of a case and literature review
M Wahiduzzaman MBBS Dip-Derm (S'pore & UK), M Pubalan MBBS MRCP (UK).DGUM (UK)
Dermatology Online Journal 14 (12): 14
Department of Dermatology, Sarawak General Hospital, Jalan Tun Ahmed Zaidi Adruce, 93586 Kuching, Sarawak, Malaysia. jhota68@hotmail.comAbstract
Imatinib mesylate - Gleevec® (US), Glivec® (worldwide), STI571 - is an oral cancer drug that selectively inhibits several protein tyrosine kinases associated with human malignancy. The drug is used for the treatment of chronic myeloid leukemia, malignant gastrointestinal stromal tumors, and some other conditions. Treatment with imatinib is generally well tolerated but not without the risk of adverse effects. The risk of severe adverse events is low. Cutaneous side effects of this drug are common but muco-cutaneous lichenoid eruption with nail changes is very rare. We report a case of lichenoid eruption during imatinib therapy involving the skin, mucous membranes, and nails that cleared in spite of ongoing imatinib therapy.
Introduction
Imatinib (STI571) suppresses BCR-ABL protein, which is an active tyrosine kinase that is produced by the abnormal Philadelphia chromosome, characteristic of chronic myeloid leukemia. The drug causes competitive inhibition at the enzyme's ATP-binding site leading to inhibition of tyrosine phosphorylation of proteins involved in BCR-ABL signal transduction [1]. Because of the excellent clinical response in chronic myeloid leukemia (CML) the drug has recently been approved as a first line treatment for CML patients. Because the drug is orally available, has a high hematological and cytogenetic response, and has variable well- tolerated adverse effects, it has become the gold standard for treatment of CML [2]. Adverse skin reactions resulting from imatinib have been well described. However, reports of associated lichenoid skin eruption with mucosal involvement and nail changes in a single patient are exceedingly rare. From our extensive literature search we have found five cases with lichenoid skin rash [3, 4, 5, 6, 7], three with oral mucosal changes [6, 8, 9] and one report of nail changes involving three patients [10] that did not involve the mucous membrane. We believe that no case involving the skin, mucous membranes, and the nails in a single patient has been reported before.
Case report
A 31-year-old male was diagnosed to have Philadelphia chromosome-positive (Ph+) chronic myeloid leukemia (CML) in June 2007 by the hematology clinic and was later reviewed by the dermatology clinic in December 2007 for his skin problem. He presented with generalized pruritic violaceous papules, nodules and plaques symmetrically involving the chest, palms, arms, soles, legs, and thighs, bilaterally. He was also noted to have involvement of the lips, buccal mucosa, tongue, and genitalia. The mucosal plaques exhibited a lattice pattern. One of his fingernails developed longitudinal ridging (Figs. 1-5). The lesions on the skin were very itchy in nature. He had been treated with imatinib mesylate 400 mg daily for 5 months before the onset of the eruption. Prior to initiation of imatinib he had been given hydroxyurea for about a month. This medication was stopped when he started imatinib. He had no history of any previous drug allergy and was not taking any other medications.
 |  |
| Figure 1a | Figure 1b |
|---|---|
| Figures 1a & 1b. Violaceous papules, plaques, and nodules violaceous in color | |
 |  |
| Figure 2a | Figure 2b |
|---|---|
| Figures 2a & 2b. Lesions on both soles and dorsum of the feet | |
 |  |
| Figure 3a | Figure 3b |
|---|---|
| Figures 3a & 3b. Lesions on lips and tongue | |
 |  |
| Figure 4a | Figure 4b |
|---|---|
| Figures 4a & 4b. Buccal mucosal lesions showing lattice pattern | |
 |
| Figure 5 |
|---|
| Figure 5. Nail ridging on the right index finger |
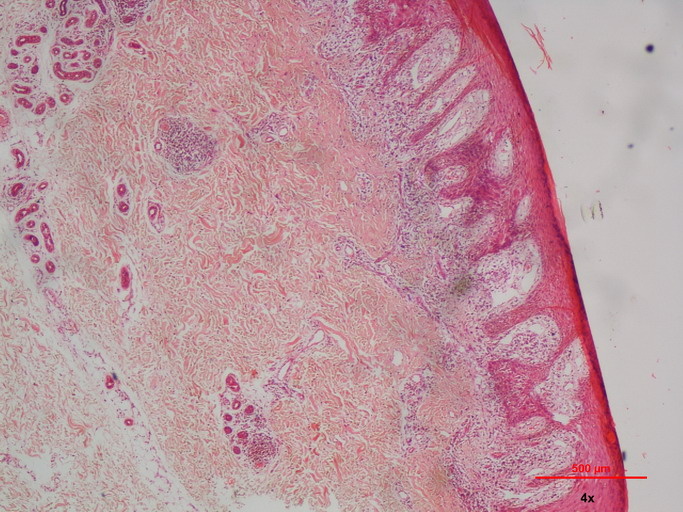
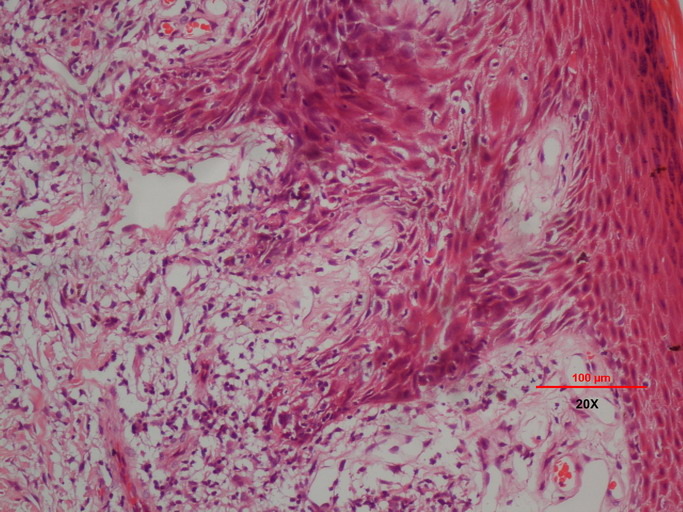
A 4 mm punch biopsy of a papule from the right arm was taken. Histopathological examination showed hyperkeratosis with irregular acanthosis and saw tooth appearance of the rete-ridges. Basal cell degeneration with infiltration of the epidermis with lymphocytes and colloid bodies were noted. The upper dermis showed a lichenoid band-like heavy infiltration with lymphocytes and scattered eosinophils. A perivascular infiltrate with lymphocytes was also noted (Figs. 6-8).
 |  |
| Figure 6 | Figure 7 |
|---|---|
| Figure 6. Scanning view exhibits hyperkeratosis with irregular acanthosis, a band like lymphocyte infiltration in the upper
dermis Figure 7. Basal cell degeneration with infiltration | |
 |
| Figure 8 |
|---|
| Figure 8. Scattered eosinophils |
The histological picture of our biopsy is most likely to be consistent with a lichenoid drug eruption because of imatinib. The histological findings may look like classical LP; supportive histological characteristics for a lichenoid drug eruption include focal parakeratosis, the presence of eosinophils, exocytosis of lymphocytes into the upper epidermis and a deep perivascular infiltrate [11]. Post biopsy he was treated initially with oral prednisolone 30 mg OD for one week which was extended to one more week with very good clinical response (Figs. 9-14). Topically he received Elomet cream (Mometasone furoate 0.1%) later changed to Dermovate (Clobetasol propionate 0.05%).Imatinib was neither stopped nor reduced as the rash was not life threatening for him and the drug was necessary for his disease remission. He continued to improve; after 2 months of treatment and maintained good clearance without any relapse of the rashes. The patient is still under our follow-up and care.
 |  |
| Figure 9 | Figure 10 |
|---|---|
| Figures 9 & 10. Images showing resolving lesions on both palms and soles with PIH | |
 |  |
| Figure 11 | Figure 12 |
|---|---|
| Figures 11 & 12. Buccal plaques are cleared at the end of 2 months | |
 |  |
| Figure 13 | Figure 14 |
|---|---|
| Figures 13 & 14. Good clearance of both the lips and tongue | |
Discussion
Imatinib therapy has changed the course of chronic myeloid leukemia (CML) and has been established as the first-line treatment in CML patients. As imatinib is increasingly used, adverse reactions to will also increase. The drug may cause mild nausea and diarrhea; this is reported to be common. Other side effects are fluid retention, muscle cramps, skin eruptions, renal and hepatic failure, and hematologic toxicity including hemolytic anemia [12, 13, 14, 15, 16].
Several types of adverse cutaneous reactions have been mentioned with imatinib and in several series were reported to be 9.5 percent to 69 percent. Rash, edema, and pruritus appear most commonly and are usually described as moderate and dose-dependent [17, 18]. Cutaneous eruptions have been described as maculopapular, erythematous, and edematous (commonly involving the periorbital region). Imatinib can also induce severe and sometimes life-threatening cutaneous reactions such as Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis [17, 19, 20, 21, 22]. There has also been a report of a pityriasis rosea-like eruption because of imatinib [23]. About five percent of cases are reported to be severe and life threatening.
Cutaneous lichenoid eruption associated with imatinib is a rare adverse event [24]. Our patient presented with generalized violaceous, pruritic eruption. The palm and sole plaques were hypekeratotic. The mucosal lesion on the buccal mucosa caused him discomfort. We initiated treatmet with oral prednisolone, 30 mg daily for two weeks; he applied potent topical corticosteroid, initially Mometasone furoate (0.1%) and later clobetasol propionate (0.05%). Our patient responded very well and after two weeks of medication the skin and the mucosal lesions resolved significantly. His itchiness also improved dramatically; by the end of two months only residual macular hyperpigmentation remained. During the follow-up visits his skin condition was stable and the lichenoid eruption did not recur. Other than mild itchiness and hyperpigmentation he did not complain of any other problems. Since the biopsy was taken in December 2007 the patient has been seen by the dermatology team on eight occasions, with the last follow-up in November 2008. During the follow-up visits he was maintained on topical corticosteroids only including the oral cavity. The patient has not required reinstitution of oral corticosteroids again.
Lichenoid drug eruptions have been reported to occur after a latent period that ranges between a few weeks to several months from administration. In our case the lichenoid eruption appeared after a period of five months, which is within the time period of the reported cases. In one series from India the eruption appeared six months after the initiation of the drug [5]. Even severe drug reactions like SJS have been reported from India to appear after six months of the drug; recurrence did not appear after re-challenge [22]. In our case the eruption was extensive but did not seem to be severe or life-threatening. In our patient imatinib was maintained at the initial dose of 400 mg daily and the drug was neither stopped temporarily nor reduced. At his most recent visit in the hematology clinic in November 2008 a bone marrow aspiration showed maintained remission. The various cutaneous eruptions to imatinib reported in the past have showed a variable response. In some cases improvement was noted without the need for suspension of drug, as in our case [3, 5, 9], Sometimes imatinib administration had to be stopped transiently or permanently [3, 4].
Lichenoid drug eruption is not common with imatinib; it is even less common to have both skin and mucosal involvement and rare to have nail involvement. Imitanib is proving to be very useful drug in CML and its use will increase. Temporary dose reduction or discontinuation of drug may be required in the event of severe cutaneous eruptions. However, the lichenoid eruption exhibited by our patient was easily manageable with a short course of oral corticosteroids and topical corticosteroid. Once he improved topical corticosteroid alone was adequate to maintain clearing.
Acknowledgement: We acknowledge and thank Dr. Nurshaline Pauline Hj. Kipli, BDS(Dundee), FDSRCS(ENG) for her help in obtaining the photomicrography of the HPE slide from her department.
References
1. Druker BJ, Talpaz M, Resta DJ, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N Engl J Med 2001; 344(14):1031-7. [PubMed].2. Peggs K, Mackinnon S. Imatinib Mesylate--the new gold standard for treatment of chronic myeloid leukemia. N Engl J Med 2003; 348:1048-50. [PubMed].
3. J Dalmau, L Peramiquel, L Puig, M T Fernández-Figueras MT, Roé A Alomar. Imatinib-associated lichenoid eruption: acitretin treatment allows maintained antineoplastic effect. Br J Dermatol Jun 2006 (Vol. 154, Issue 6, Pages 1213-6. DOI 10.1111/j.1365-2133.2006.07276.x
4. Davin Lim, James Muir. Lichenoid eruption to STI 571.Am J Hematol Jun 2002 (Vol. 70, Issue 2, Page 179). [PubMed].
5. Prabhash K, Doval DC. Lichenoid eruption due to imatinib. Indian J Dermatol Venereol Leprol 2005; 71:287-8. [PubMed]
6. Pascual JC, Matarredona J, Miralles J, Conesa V, Borras-Blasco J. Oral and cutaneous lichenoid reaction secondary to imatinib: report of two cases. Int J Dermatol Dec 2006 (Vol. 45, Issue 12, Pages 1471-3). [PubMed]
7. Chan CYS, Browning J, Smith-Zagone MJ et al, Cutaneous Lichenoid dermatitis associated with imatinib mesylate. Dermatology Online Journal. 2007; 13(2): 1087-2108. [PubMed]
8. D S Lim, James Muir Dermatology 2002 (Vol. 205, Issue 2, Pages 169-71). [PubMed].
9. Ena P, Chiarolini F, Siddi GM, Cossu A. Oral lichenoid eruption secondary to imatinib (Glivec). J Dermatolog Treat 2004; 15:253. [PubMed].
10. N. Deguchi, T. Kawamura, A. Shimizu, R. Kitamura et al. Imatinib mesylate causes palmoplantar hyperkeratosis and nail dystrophy in three patients with chronic myeloid leukaemia. : Br J Dermatol. 2006 Jun; 154(6):1216-8. [PubMed].
11. Van Den Haute V, Antoine JL, Lachapelle JM. Histopathological discriminant criteria between lichenoid drug eruption and idiopathic lichen planus: retrospective study on selected samples. Dermatologica. 1989; 179(1):10-3. [PubMed].
12. Hande KR. Principles and Pharmacology of Chemotherapy. In Greer JP, Foerster J, Lukens JN, Rodgers GM, Paraskevas F, Glader B (eds); Wintrobe's Clinical Hematology, 11th Edition, Volume II, Part VII, Ch: 73, pp: 1945-1969, Lippincott Williams & Wilkins Co. Philadelphia 2003.
13. Wetzler M, Byrd JC, Bloomfield CD. Acute and Chronic Myeloid Leukemia. In Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL (eds). Harrison's Principles of Internal Medicine. 16th Edition, Part: V, Ch: 96, pp: 631-641. McGRAW - HILL Co. New York 2005.
14. Foringer JR, Verani RR, Tjia VM, Finkel KW, Samuels JA, Guntupalli JS. Acute renal failure secondary to imatinib mesylate treatment in prostate cancer. Ann Pharmacother 2005; 39:2136-8. [PubMed].
15. Cross TJ, Bagot C, Portmann B, Wendon J, Gillett D. Imatinib mesylate as a cause of acute liver failure. Am J Hematol 2006; 81:189-92? [PubMed].
16. De Arriba JJ, Nerín C, García E, Gomez-Aldaraví L, Vila B. Severe hemolytic anemia and skin reaction in a patient treated with imatinib. Ann Oncol 2003; 14:962. [PubMed].
17. Valeyrie L, Bastuji-Garin S, Revuz J, Bachot N, Wechsler J,Berthaud P, et al. Adverse reactions to imatinib in Philadelphia chromosome-positive leukemias: A prospectivestudy of 54 patients. J Am Acad Dermatol2003; 48:201-6. [PubMed].
18. Brouard M, Saurat JH. Cutaneous reactions to STI571. N Engl J Med. 2001 Aug 23; 345(8):618-9. [PubMed].
19. Scheinfeld N. Imatinib Mesylate and dermatology part 2: a review of the cutaneous side effects of imatinib Mesylate. J Drugs Dermatol 2006; 5:228-31. [PubMed].
20. Hsiao LT, Chung HM, Lin JT, Chiou TJ, Liu JH, Fan FS, Wang WS, Yen CC, Chen PM. Stevens-Johnson syndrome after treatment with STI571: a case report. Br J Haematol 2002; 117: 620-2. [PubMed].
21. Schaich M, Schakel K, Illmer T, Ehninger G, Bornhauser M. Severe epidermal necrolysis after treatment with imatinib and consecutive allogeneic hematopoietic stem cell transplantation. Ann Hematol 2003; 82:303-4. [PubMed].
22. Pavithran Keechilat, Thomas Mathew. Imatinib induced Stevens-Johnson syndrome: lack of recurrence following re-challenge with a lower dose.Indian Journal of Dermatology, Venereology and Leprology, Vol. 71, No. 4, July-August, 2005, pp. 288-289. [PubMed].
23. Brazzelli , F . Prestinari , E . Roveda , T . Barbagallo et al , Pityriasis rosea-like eruption during treatment with imatinib mesylate: description of 3 cases Journal of the American Academy of Dermatology , Volume 53 , Issue 5 , Pages S240 - S243 V . [PubMed].
24. Roux C, Boisseau-Gersaud AM, Saint-Cyr I, Hekenon R, Quist D, Delaunay C. Lichenoid cutaneous reaction to imatinib. Ann Dermatol Venereol 2004; 131:571-3. [PubMed].
© 2008 Dermatology Online Journal