Leprous osteitis presenting as bone cyst and erosions
Published Web Location
https://doi.org/10.5070/D314h8k0t1Main Content
Leprous osteitis presenting as bone cyst and erosions
Shriya Dave1 Achyuta V Nori1, Devinder M Thappa1, N Siddaraju2
Dermatology Online Journal 10 (1): 17
Department of Dermatology and STD1, and Department of Pathology2, Jipmer, Pondicherry, India. dmthappa@vsnl.net
Abstract
A 30-year-old man presented to the Hansen outpatient department with swelling and ulceration of toes for 2 months and swelling of the right fifth and fourth fingers and the left second finger for 1 month. In addition to skin lesions of lepromatous leprosy (subpolar type), there was nontender, non-fluctuant swelling of the right fifth and fourth fingers and left second finger. Skin over the right fifth finger showed sinus-like openings with associated purulent discharge. He also had swelling and ulceration of second left toe. Slit-skin smear (SSS) showed a bacterial index of 6+ from the ear lobes and cutaneous nodules, 4+ from the patch, and 3+ from normal skin. Modified Ziehl-Neelsen staining of the discharge extruding from the sinuses on the right fifth finger also showed abundant acid-fast bacilli. Radiography of the hands and feet showed lytic lesions in the distal epimetaphyseal region of proximal phalanx of the right fifth finger and left second finger and erosion of distal end of proximal phalanges of both second toes. Histopathological examination of biopsy specimen from the patch (back) showed features of lepromatous leprosy, and Fite-Faraco stain for tissue acid-fast bacteria (AFB) was strongly positive. Fine-needle-aspiration cytology (FNAC) from the lytic lesion in the bone also showed predominantly foamy macrophages with strongly positive staining for AFB with a few interspersed lymphocytes, epithelioid cells and Langhans giant cells. On the basis of these features, a clinical diagnosis of subpolar lepromatous leprosy with leprous osteitis was made. In today's clinical era of improved case detection and prompt treatment with effective multidrug regimens, advanced bone changes are rarely encountered. We describe this case of lepromatous leprosy that developed cavitating lesions of the phalanges of the hand, seen on x-ray as well-defined bone cyst and erosions.
Introduction
Bone changes in leprosy occur in a high percentage of cases and account for much physical disability and psychosocial distress in these patients. Various studies have shown incidence of overall bone changes in leprosy to be ranging from 82.9 percent to 91 percent [1]. The common sites of predilection for bone damage in leprosy are the small bones of hands and feet followed by bones of the face [1, 2]. In today's clinical era of improved case detection and prompt treatment with effective multidrug regimens, advanced bone changes are rarely encountered. We describe a patient with lepromatous leprosy who developed cavitating lesions of the phalanges of the hand, seen on x-ray as well-defined bone cyst and erosions.
Case report
A 30-year-old man presented to the Hansen outpatient department with swelling and ulceration of the toes for the prior 2 months and swelling of the right fifth finger and fourth finger and the left second finger for the prior 1 month. He also gave history of occasional epistaxis for the past 2 months. There was history of thermal burns on the toes, which had left nonhealing ulcers. The patient had been diagnosed as having leprosy 11 years prior when he had developed hypopigmented, hypoanesthetic patches over the hands and thighs and had been subsequently started on multibacillary (MB) multidrug therapy (MDT). However, he had defaulted treatment after 1 month. There was no prior history suggestive of lepra reaction (type 1 or type 2). On examination, there were large hypopigmented to copper-colored ichthyotic patches with well to ill-defined margins and decreased pain sensation over extensor aspect of both forearms and lower limbs (extending from foot to knee). Multiple papules and a few nontender, nonevanescent nodules were present on the back. There was bilateral pitting pedal edema and nontender, nonfluctuant swelling of the right fifth and fourth fingers and left second finger (figs. 1-3). Skin over the right fifth finger showed sinus-like openings with purulent discharge. He also had swelling and ulceration of the second left toe (fig. 4). The right greater auricular nerve, bilateral ulnar nerves, bilateral radial cutaneous nerves, and right common peroneal nerves were thickened uniformly and were nontender. There was bilateral patchy glove-and-stocking anesthesia.

|

|
| Figure 1 | Figure 2 |
|---|---|
| Hands showing swelling of the right fifth and fourth fingers and left second finger (fig. 1). | |
| Right fifth finger showing swelling and sinus openings (fig. 2). | |

|

|
| Figure 3 | Figure 4 |
|---|---|
| Right second finger dactylitis with sinuses (fig. 3). | |
| Left second toe with ulceration (fig. 4). | |
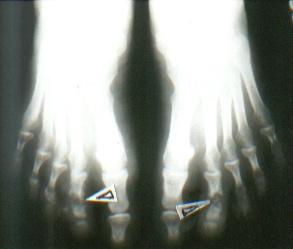
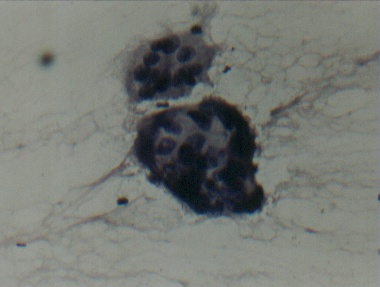
Slit-skin smear (SSS) showed a bacterial index of 6+ from the ear lobes and cutaneous nodules, 4+ from the patch and 3+ from normal skin. Modified Ziehl Neelsen staining of the discharge extruding from the sinuses on the right fifth finger also showed abundant acid-fast bacilli. Radiography of the hands showed lytic lesions in the distal epimetaphyseal region of proximal phalanx of the right fifth finger and left second finger and erosion of distal end of proximal phalanges of both second toes (figs. 5 and 6). Histopathological examination of biopsy specimen from the patch on the back showed features of lepromatous leprosy, and Fite-Faraco stain for tissue AFB was strongly positive. Fine-needle aspiration cytology (FNAC) from the lytic lesion in the bone also showed predominantly foamy macrophages with strongly positive staining for AFB with a few interspersed lymphocytes, epithelioid cells and Langhan giant cells (figs. 7 and 8).

|
|
| Figure 5 | Figure 6 |
|---|---|
| X-ray of the hands showing lytic lesions in the distal epimetaphyseal region of proximal phalanx of the right fifth finger and left fourth finger (fig. 5). | |
| X-ray of the feet showing erosion of distal end of proximal phalanges of both second toes (fig. 6). | |

|
|
| Figure 7 | Figure 8 |
|---|---|
| Fine needle aspiration cytology (FNAC) demonstrating foamy macrophages along with epithelioid cells (fig. 7). | |
| FNAC smear showing two giant cells (fig. 8). | |
Based on these features, a clinical diagnosis of subpolar lepromatous leprosy with leprous osteitis was made. The patient was started on WHO MB MDT along with supportive measures including nonsteroidal anti-inflammatory drugs, physiotherapy, and splinting as appropriate.
Discussion
An accurate estimate of bone changes in leprosy is not possible as most surveys deal with institutional cases rather than being truly population-based studies. Various studies have shown incidences of 34 [3], 29 [4], and 87.3 percent [1]. Bone changes in leprosy can be broadly classified into the following types:
- Specific leprous osteitis (resulting direct invasion of bones by M. leprae) [1]
- Nonspecific leprous osteitis in which the fundamental cause is damage to the nerve supply with superadded factors including vascular changes, trauma, and secondary infection [1].
- Osteoporosis, which may result from disuse, vascular changes, and local inflammation [3].
Specific bone changes owing to direct invasion by M. leprae include formation of bone cysts, honeycombing, enlarged nutrient foramina, subarticular erosion, concentric cortical erosions, and primary periosteitis [1, 3]. Healing is characterized by sclerosis. These lesions of specific leprous osteitis usually occur in very advanced cases of lepromatous leprosy of long-term duration with high bacterial indices (BI). Faget and Mayoral [2] also found that specific bone lesions are generally a late manifestation of the disease. This fact was also true in our case who had long standing Hansen's disease of 11 years duration and a high BI of 4-6+.
Specific leprous osteitis or osteomyelitis (as termed by Job et al [2]) is basically a granulomatous process very similar to chronic osteomyelitis caused by Mycobacterium tuberculosis. Histologically, affected bones show bony trabeculae invaded by granulation tissue comprised of foamy pink macrophages with abundant acid-fast bacilli, lymphocytes, and occasional plasma cells. Fragmentation and necrosis of the bony trabeculae is also evident. The granulation tissue invades into the cortex of the bone as tongue-like processes and gradually destroys the bony trabeculae with subsequent absorption leading to formation of carious lesions. Newly formed osteoid tissue is also destroyed. Healing occurs with dense fibrosis. [2]
It has been mentioned that infection is carried to the bones by the vascular supply and stated that marked destruction and cystic degeneration may follow. [4] Curettings from such a lesion have been found to be teeming with acid-fast bacilli, and Chhabriya et al. coined the term osteitis leprosa multiplex cystica to describe these lesions. Such cysts are usually multiple and are more frequent in lepromatous than non-lepromatous patients. They had also been observed earlier by other investigators [1, 5] and reported to heal if treated early with antileprosy therapy.
Our case, classified as belonging to the lepromatous spectrum, had specific leprous osteitis affecting the phalanges. The presence of lytic lesions on scintigraphy along with demonstration of AFB in the discharge from the fingers and in the FNAC specimen confirmed that the bone changes were indeed a result of direct invasion by M. leprae. The presence of epithelioid cells and giant cells in the FNAC specimen could be probably because the patient had begun his disease 11 years prior in the borderline tuberculoid spectrum (suggested by the morphology of the initial patches) and subsequently downgraded to the lepromatous pole in the absence of treatment. Striking in our case was the presence of frank sinuses discharging pus, teeming with AFB, and overlying the affected phalanges. Findings of such frank, florid leprous osteomyelitis are indeed rare in the present era and pose a serious question mark regarding our case detection and treatment strategies. Are we probably underestimating the pathogenicity of this organism?
References
1. Choudhuri H, Thappa DM, Kumar RH, Elangovan S. Bone changes in leprosy patients with disabilities/deformities (a clinico-radiological correlation). Indian J Lepr. 1999 Apr-Jun;71(2):203-15. PubMed2. Job CK. Pathology of leprous osteomyelitis. Int J Lepr. 1963 Jan-Mar;31:26-33. PubMed
3. Paterson DE. Bone changes in leprosy, their incidence, progress, prevention and arrest. Int J Lepr. 1961 Oct-Dec;29:393-422. PubMed
4. Lechat MF. Bone lesions in leprosy. Int J Lepr. 1962 Apr-Jun;30:125-37. PubMed
5. Chhabriya BD, Sharma NK, Aggarwal GR. Bone changes in leprosy. A study of 50 cases. Indian J Lepr. 1985 Jul-Sep;57(3):632-9. PubMed
© 2004 Dermatology Online Journal