Cutaneous metastasis of renal cell carcinoma: A case report
Published Web Location
https://doi.org/10.5070/D313h735rkMain Content
Cutaneous metastasis of renal cell carcinoma: A case report
Hamid Reza Mahmoudi1 MD, Kambiz Kamyab2 MD, Maryam Daneshpazhooh1 MD
Dermatology Online Journal 18 (5): 12
1. Autoimmune Bullous Diseases Research Center, Tehran University of Medical Sciences, Tehran, Iran. daneshpj@tums.ac.ir2. Department of Pathology, Tehran University of Medical Sciences, Tehran, Iran
Abstract
Cutaneous metastasis develops in 5 to 10 percent of high-stage cancer patients. About 6 percent of cutaneous metastases are caused by renal cell carcinomas (RCC). A 64-year-old man presented with a 4-month history of a rapidly enlarging lesion on the mental region. There was a 2 cm x 3 cm multilobular and polypoid angiomatous tumor in the center of the swelling. Histopathologic examination revealed clear cell proliferation with gland formation and red blood cell (RBC) extravasation, compatible with metastatic renal cell carcinoma. The rich vascular structure of RCCs facilitates hematogenous extension and the development of distant metastasis. Arteriovenous and systemic shunts are thought to facilitate the tumor cells’ path to the head and neck region. RCC cutaneous metastasis is known to have a vascular appearance. It is important to consider RCC metastasis in the differential diagnosis of new onset tumors with a vascular appearance in the head and neck region.
Introduction
Cutaneous metastasis is a rare condition, but may be the presenting sign of malignancy and historically signifies a bad prognosis [1]. Cutaneous metastasis develops in 5 to 10 percent of high-stage cancer patients, most frequently with cancers of the breast, lung, colon, and ovary, in addition to malignant melanoma [2].
Renal cell carcinoma (RCC) is known as a highly aggressive tumor, which requires early diagnosis to optimize the chance of cure [3]. RCCs are have the potential to metastasize to the lymph nodes, lungs, liver, opposite kidney, adrenal glands, brain, and bone [4].
Given the distance from the anatomical origin, the development of RCC-related cutaneous metastasis in the head and neck would seem unusual. We report a case of facial metastasis of RCC in an old man.
Case report
 |
| Figure 1 |
|---|
| Figure 1. Swelling in mental region with a 2 cm x 3 cm multilobular and polypoid angiomatous tumor in the center of the swelling |
A 64-year-old man presented with a 4-month history of a rapidly enlarging nodule on the mental region. He mentioned a history of an 8 kg weight loss within 3 months. The lesion was a 6 cm x 7 cm swelling in the mental region and lower lip with a firm consistency. There was a 2 cm x 3 cm multilobular and polypoid angiomatous tumor in the center of the swelling. There was a 1 cm x 2 cm mass with a firm consistency in the inner aspect of the lower lip, in the vicinity of the tumor (Figure 1). He had a history of right radical nephrectomy 2 years prior to presentation; the pathology report was compatible with renal cell carcinoma – clear cell type. No further treatment had been performed.
A 1 cm x 1 cm incisional biopsy was performed from the cutaneous nodule. Our clinical differential diagnoses included metastasis, angiosarcoma, Kaposi sarcoma, pyogenic granuloma, and amelanotic melanoma.
 |  |
| Figure 2 | Figure 3 |
|---|---|
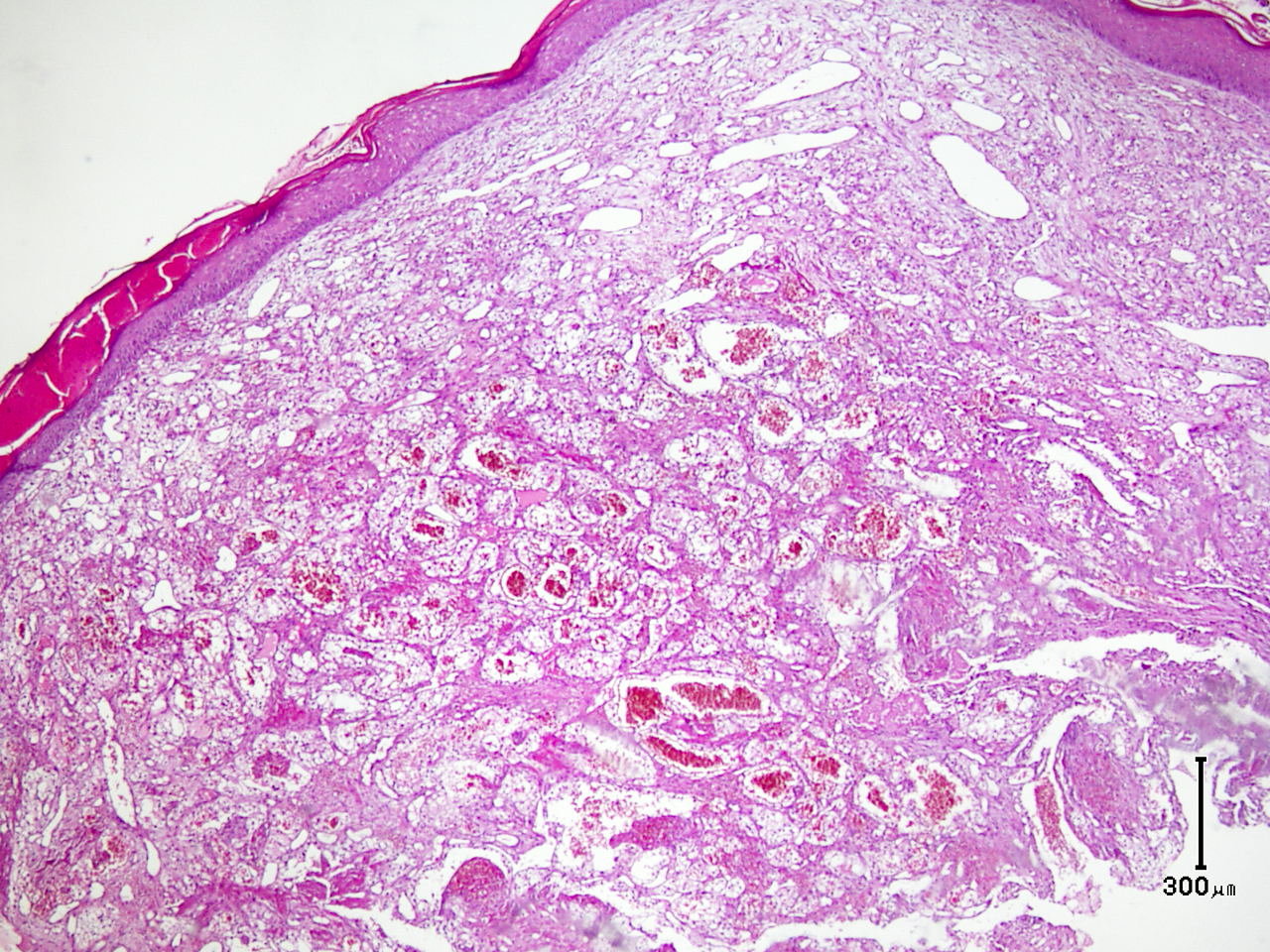
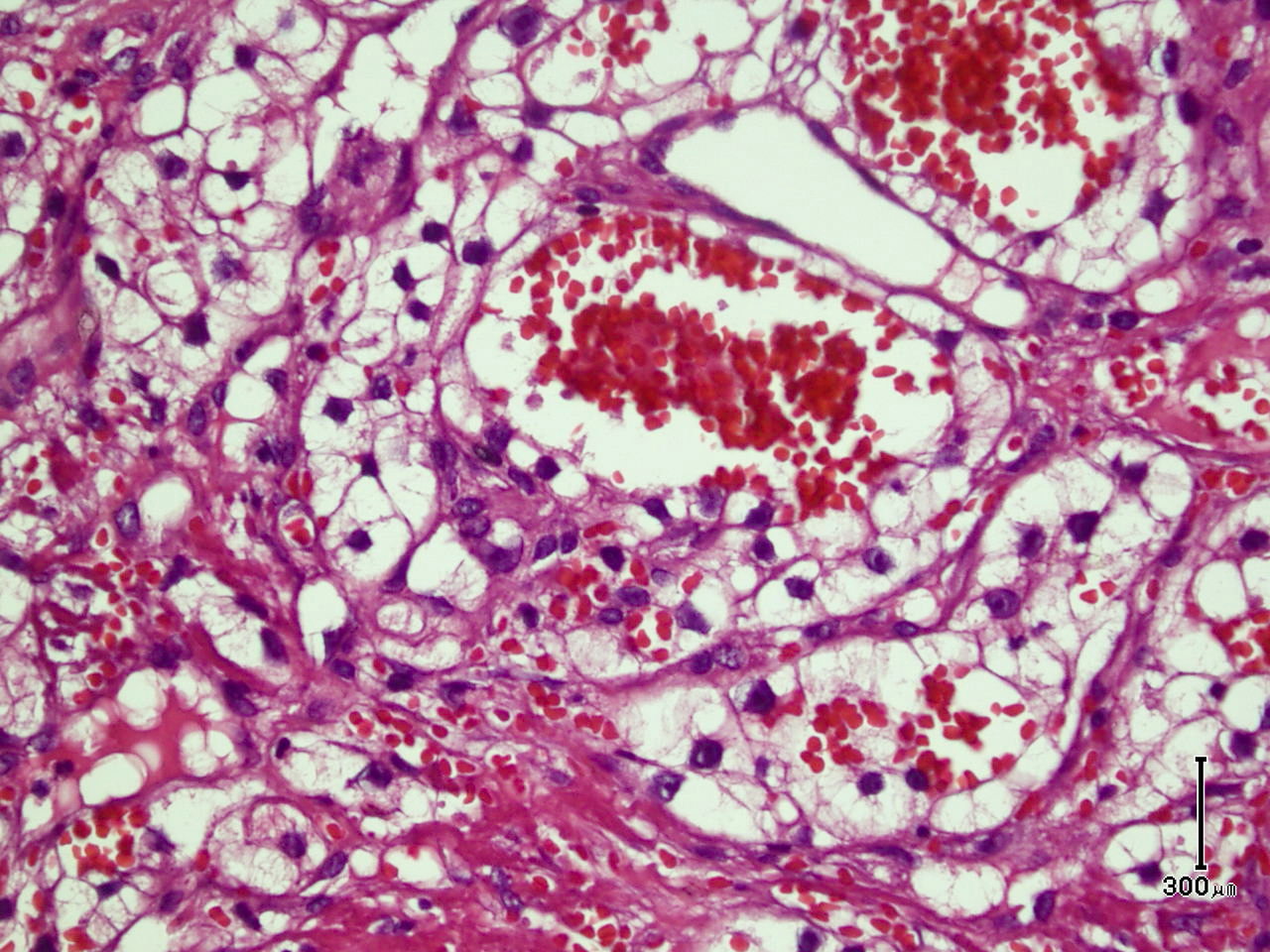
| Figure 2. Clear cell proliferation expanding the dermis Figure 3. Clear cell proliferation with gland formation and prominent RBC extravasation | |
Histopathologic examination revealed an expanded dermis by clear cell proliferation with gland formation and prominent RBC extravasation, compatible with metastatic renal cell carcinoma (Figures 2 and 3). Immunohistochemical testing revealed that the tumor cells reacted positively with vimentin, cytokeratin, and partially to CD10, which was in favor of metastatic renal cell carcinoma.
Our patient was referred to an oncologist. Upon further evaluation there were several metastatic lesions in the lung and mediastinum shown by CT scan study. The patient underwent chemotherapy with sorafenib and sunitinib, accompanied by radiotherapy for the cutaneous lesion. After about 10 months the patient is still alive.
Discussion
Renal cell carcinomas comprise 2 to 3 percent of all adult malignancies. The classical sign of RCC, including hematuria, flank pain, and palpable abdominal mass are detected in only 10 percent of RCC cases. Consequently, most patients are diagnosed during examination for other situations or by appearance of metastatic lesions [5].
Cutaneous metastases form 2.8 to 4.4 percent of skin malignant carcinomas. About 6 percent are caused by renal cell carcinomas [6]. Regarding the cutaneous metastasis of renal carcinoma described in the literature, the most common site was the scalp, followed by the abdominal region [7].
Various mechanisms are described for cutaneous metastasis of visceral malignancies. The most frequent is the direct invasion of the skin tissue covering the malignant mass [8].
The rich vascular structure of RCCs facilitates hematogenous extension and the development of distant metastases. The most important hematogenous extension route in RCC is the vena cava system, which leads to the lung. Arteriovenous and systemic shunts are thought to facilitate the tumor cells’ path to the head and neck region. Tumor-related growth factors such as parathormone-related protein and truncated fibronectin growth factor may play a role in the localization of cutaneous metastasis in this region [8]. The differential diagnoses of cutaneous RCC metastatic lesions are: sebaceous carcinoma, sweat gland tumor, and melanoma [9]. Renal cell carcinoma cutaneous metastasis is known to have a vascular appearance [1] and should be differentiated from pyogenic granoluma [10], Kaposi sarcoma, angiosarcoma, and other vascular tumors by histopathology.
The development of cutaneous metastasis in RCC is associated with poor prognosis and most patients die within 6 months of metastasis detection. Therefore the treatment options are limited and mostly palliative.
Two points are worth mentioning in our patient: First of all, the cutaneous metastasis heralded the detection of visceral metastasis of RCC. This further emphasizes the role of skin examination in the follow-up of known patients with this malignancy. On the other hand, despite the known poor prognosis of patients with RCC metastases, our patient is still surviving at the time of this report. This may be partly due to the role of the new drugs used in this setting.
Therefore, it is important to consider RCC metastasis in the differential diagnosis of new onset nodules, ulcers, or tumors with a vascular appearance in the head and neck, especially in a patient with a past medical history of renal tumor.
References
1. Davis D, Pellowski D. Cutaneous metastasis In: Bolognia JL, Jorizoo JL, Rapini RP. Dermatology (Callen JP, Horn TD, Mancini AJ et al, eds) 2nd edition. Spain, Elsevier, 2008: 1897-19012. Lookingbill DP, Spangler N, Helm KF. Cutaneous metastases in patients with metastatic carcinoma: a retrospective study of 4020 patients. J Am Acad Dermatol. 1993 Aug;29(2 Pt 1):228-36. [PubMed]
3. Novick AC, Campbell SC. Renal Tumors. In: Walsh P C., Retik A B. Vaughan ED. Jr, Wein AJ. Campbell’s Urology, 8th Edition. Philadelphia, Saunders, 2002: 2672-731.
4. Ather MH, Masood N, Siddiqui T. Current management of advanced and metastatic renal cell carcinoma. Urol J. 2010 Winter;7(1):1-9. [PubMed]
5. Weiss L, Harlos JP, Torhorst J et al. Metastatic patterns of renal carcinoma: an analysis of 687 necropsies. J Cancer Res Clin Oncol. 1988; 114(6):605-12. [PubMed]
6. White JW. Evaluating cancer metastatic to the skin. Geriatrics. 1985 Aug; 40(8):67-73. [PubMed]
7. Brownstein MH, Helwig EB. Patterns of cutaneous metastasis. Arch Dermatol. 1972 Jun; 105(6):862-8. [PubMed]
8. Onak Kandemir N, Barut F, Yılmaz K et al. Renal cell carcinoma presenting with cutaneous metastasis: a case report, Case Report Med. 2010;2010. pii: 913734. Epub 2010 Aug 2. [PubMed]
9. Hugo HS. Cancer. In: McPhee SJ, Papadakis MA, editors. Current medical diagnosis and treatment, 48th ed. 2009:1463-4, 1489-90.
10. Batres E, Knox JM, Wolf JE Jr. Metastatic renal cell carcinoma resembling a pyogenic granuloma. Arch Dermatol. 1978 Jul; 114(7):1082-3. [PubMed]
© 2012 Dermatology Online Journal