Generalized discoid lupus erythematosus
Published Web Location
https://doi.org/10.5070/D30t23n449Main Content
Generalized discoid lupus erythematosus
Rachel Farley-Loftus MD, Matthew Mahlberg MD, Joseph F Merola MD, Henry J Votava MD, Shane Meehan MD, Jennifer Stein MD PhD,
Jerome L Shupack MD
Dermatology Online Journal 15 (8): 18
Department of Dermatology, New York UniversityAbstract
A 79-year-old woman presented with a four-year history of generalized, erythematous, indurated plaques on the malar areas, back, and extremities. The lesions had been recalcitrant in the past to topical glucocorticoid therapy. A skin biopsy specimen was diagnostic of discoid lupus erythematosus (DLE). A minority of patients with DLE progress to develop systemic lupus erythematosus although generalized DLE is more frequently associated with systemic involvement than is limited disease. Standard therapy of cutaneous lupus includes broad spectrum sunscreens, topical and intralesional glucocorticoids, and antimalarial agents.
History
 |  |
| Figure 1 | Figure 2 |
|---|---|
 |
| Figure 3 |
|---|
A 79-year-old woman was hospitalized at New York University Langone Medical Center in February, 2009, for an acute cerebrovascular accident. During this admission, the Dermatology Service was consulted to evaluate a generalized, pruritic skin eruption on the face, extremities, and trunk. The eruption had followed a variable course since its initial onset four years earlier. Skin biopsies had been performed in the past. Several unspecified topical therapies had been prescribed during this time although none had resulted in clinical improvement.
Past medical history included previous abdominal surgery. She denied a personal or family history of photosensitivity or connective-tissue disease.
A punch biopsy was performed.
Physical Examination
There were blanching, erythematous, indurated plaques without scale on the malar eminences, which spared the nasolabial folds and involved the eyelid margins. Similar plaques were somewhat symmetrically distributed and involved an extensive surface area along the upper back, extensor aspects of the arms, dorsal aspects of the hands, and extensor aspects of the legs. No conjunctival or oral mucosal lesions were present. No joint swelling or tenderness was noted.
Laboratory data
A complete blood count, basic metabolic panel, hepatic function profile, prothrombin time, and partial thromboplastin time were normal. Urinalysis contained leukocytes. C-reactive protein was 15mg/dL. Anti-nuclear antibody titer was less than 40. Anti-double-stranded DNA, SS-A, SS-B, Smith, and ribonucleoprotein antibodies were not detected. Complement levels and aldolase were normal. A rapid plasma regain test was non-reactive.
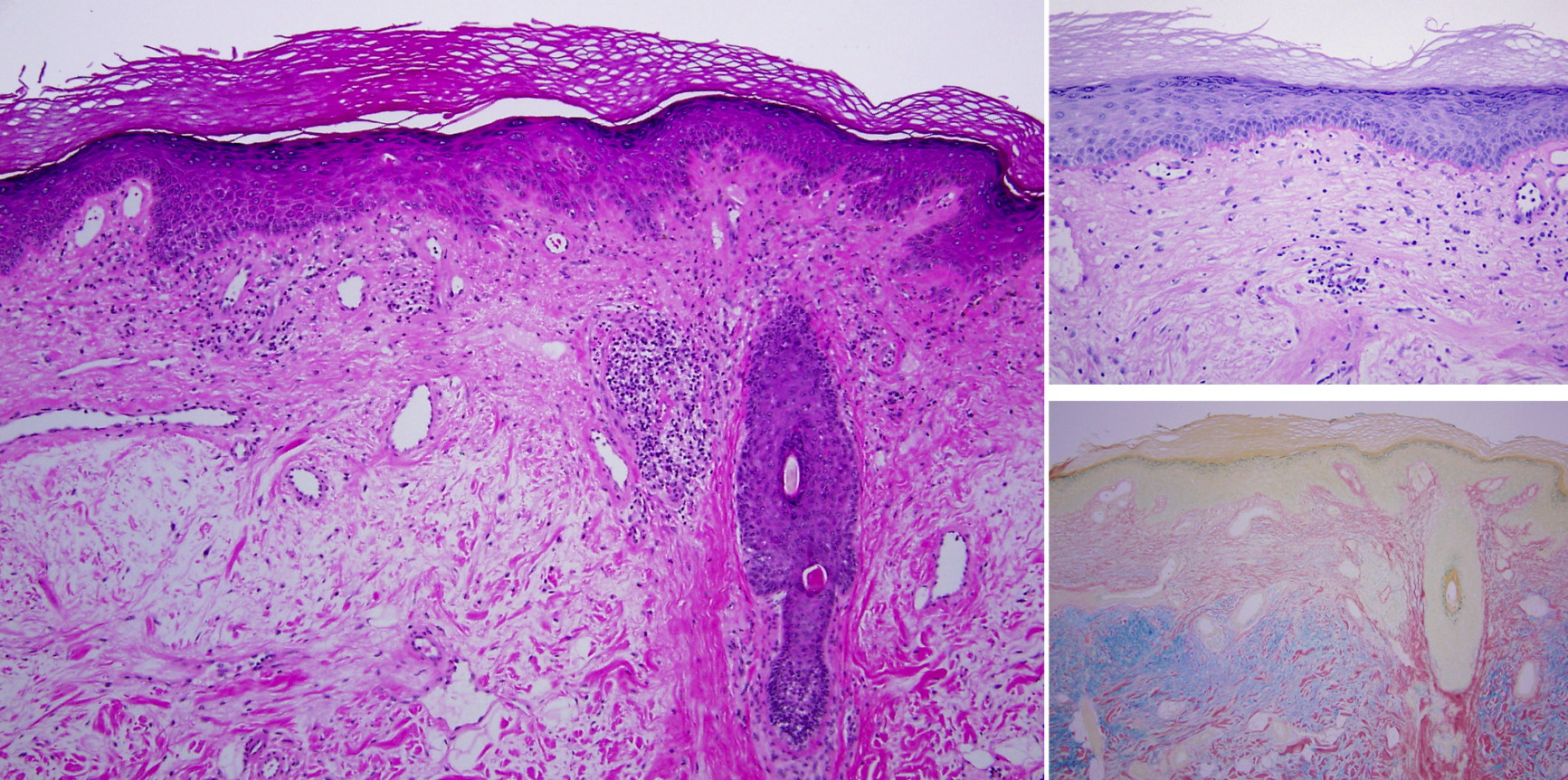
Histopathology
There is epidermal thinning with hyperkeratosis, vacuolar alteration of the basal layer, and a superficial and deep, perivascular and periadnexal lymphocytic infiltrate. A periodic acid-Schiff stain shows a thick basement membrane, and a colloidal iron stain shows increased deposits of connective-tissue mucin.
Comment
Discoid lupus erythematosus (DLE) is the most common form of chronic cutaneous lupus erythematosis according to the classification proposed by Gilliam [1, 2]. Typically, discoid lupus is characterized by erythematous macules, papules, and plaques with telangiectases, scale, and follicular plugs, which results in a scaring process with atrophy and dyspigmentation [3]. Lesions often are localized to the face, nose, and ears; may be generalized; and may or may not be restricted to sun-exposed skin. Photosensitivity is observed in 50 percent of patients [2, 4].
A small subset (5-10 percent) of patients with DLE have coexistent systemic disease. Progression to systemic lupus erythematosus (SLE) occurs with greater frequency in the setting of disseminated or generalized discoid lesions and often occurs within one to three years after diagnosis [2, 4]. Patients with localized disease tend to have fewer systemic manifestations and have a 50 percent chance of remission. Conversely, fewer than 10 percent of patients with generalized DLE experience remission [2].
Histopathologic features include an interface dermatitis with a superficial and deep, perivascular and periadnexal infiltrate that is composed primarily of lymphocytes. Liquefaction degeneration of basal keratinocytes with melanin incontinence, increased dermal deposition of mucin, and diffuse thickening of the basement membrane are observed. Follicular plugs may be prominent in discoid lesions [5]. Immunoglobulins and complement proteins are deposited in a granular distribution along the dermal-epidermal junction of lesional skin in up to 90 percent of cases of chronic cutaneous lupus erythematosus [6].
In photosensitive cutaneous lupus, ultraviolet light is hypothesized to induce apoptosis of keratinocytes, which results in increased autoantigen display, increased local cytokine release, activation of dendritic cells and T-lymphocytes, and autoantibody-mediated tissue injury [3]. Other proposed mechanisms for the development of lupus erythematosus include molecular mimicry and epitope spreading in response to exposure to infectious agents [4].
Few randomized controlled trials have been completed to evaluate therapy for DLE [7]. The cornerstone of therapy includes topical and intralesional glucocorticoids, and broad-spectrum sunscreens are recommended for all patients. Antimalarial agents, such as hydroxychloroquine, chloroquine, and quinacrine, are indicated when topical or intralesional therapy fails to control skin disease [2, 4]. Second-line therapies include topical and systemic retinoids, topical calcineurin inhibitors, thalidomide, dapsone, clofazimine, gold, sulfasalazine, and immunosuppressive agents, such as azathioprine, methotrexate, and mycophenolate mofetil [2, 4, 8-19].
References
1. Gilliam JN, et al. Distinctive cutaneous subsets in the spectrum of lupus erythematosus. J Am Acad Dermatol 1981; 4:471 [PubMed]2. Callen JP. Cutaneous lupus erythematosus: a personal approach to management. Australas J Dermatol 2006;47:13 [PubMed]
3. Lin JH, et al. Pathophysiology of cutaneous lupus erythematosus. Clinic Rev Allerg Immunol 2007;33:85 [PubMed]
4. Lee LA. Lupus erythematosus. In: Bolognia J, et al, eds. Dermatology, 2nd edition, London: Mosby, 2008: 561
5. Rapini RP. Other non-neoplastic diseases. In: Practical Dermatopathology. Philadelphia: Elsevier, 2005: 223.
6. David-Bajar KM, et al. Pathology, immunopathology, and immunohistochemistry in cutaneous lupus erythematosus. Lupus 1997;6:145. [PubMed]
7. Jessop S, et al. Drugs for discoid lupus erythematosus. Cochrane Database Syst Rev 2001: CD002954 [PubMed]
8. DuBois EL. Antimalarials in the management of discoid and systemic lupus erythematosus. Semin Arthritis Rheum 1978;8:33 [PubMed]
9. Tzellos TG, et al. Topical tacrolimus and pimecrolimus in the treatment of cutaneous lupus erythematosus: an evidence-based evaluation. Eur J Clin Pharmacol 2008;64:337 [PubMed]
10. Kyriakis KP, et al. Experience with low-dose thalidomide therapy in chronic discoid lupus erythematosus. Int J Dermatol 2000;39:218 [PubMed]
11. Green SG, et al. Successful treatment of hypertrophic lupus erythematosus with isotretinoin. J Am Acad Dermatol 1987;17:364 [PubMed]
12. Edwards KR, et al. Treatment of localized discoid lupus erythematosus with tazarotene. J Am Acad Dermatol 1999;41:1049 [PubMed]
13. Lindskov R, et al. Dapsone in the treatment of cutaneous lupus erythematosus. Dermatologica 1986;172:214 [PubMed]
14. Bezerra EL, et al. Double-blind, randomized, controlled clinical trial of clofazimine compared with chloroquine in patients with systemic lupus erythematosus. Arthritis Rheum 2005;52:3073 [PubMed]
15. Dalziel K, et al. Treatment of chronic discoid lupus erythematosus with an oral gold compound (auranofin). Br J Dermatol 1986;115:211 [PubMed]
16. Artuz F, et al. Efficacy of sulfasalazine in discoid lupus erythematosus. Int J Dermatol 1996;35:746 [PubMed]
17. Shehade S. Successful treatment of generalized discoid skin lesions with azathioprine. Arch Dermatol 1986;122:376 [PubMed]
18. Goyal S, et al. Treatment of resistant discoid lupus erythematosus of the palms and soles with mycophenolate mofetil. J Am Acad Dermatol 2001;45:142 [PubMed]
19. Goldstein E, et al. Discoid lupus erythematosus: successful treatment with oral methotrexate. Arch Dermatol 1994;130:938 [PubMed]
© 2009 Dermatology Online Journal