Linear lichen planus and hepatitis C
Published Web Location
https://doi.org/10.5070/D30j52p292Main Content
Linear lichen planus and hepatitis C
María Victoria Guiote Domínguez, Anna Vilanova Mateu, Ricardo Vieira, Juan Linares Solano, Ramón Naranjo Sintes, María Teresa
Gutiérrez Salmerón
Dermatology Online Journal 12 (2): 17
Department of Dermatology, San Cecilio Hospital, Granada, Spain. viviguiote@yahoo.esAbstract
A 23-year-old man with hepatitis C was observed with brownish dome-shaped papules in a linear pattern on the chest. The papules were determined clinically and pathologically to be linear lichen planus. These lesions appeared during an interferon-alpha therapy for his hepatitis and resolved after topical treatment with tacrolimus ointment. Linear lichen planus and hepatitis C have been reported only twice previously. The association between these disorders and the potential role of interferon therapy are discussed.
Linear lichen planus represents only 0.25 percent of the different clinical patterns of the disease [1]. The first case associating disseminated lichen planus and hepatitis C was reported in 1991 [2]. This association is particularly rare with the linear pattern of lichen planus. In fact, only two reports associating hepatitis C and linear lichen planus were found in the literature, both published recently [3, 4] and occurring in patients treated with no antiviral therapy for hepatitis C.
Clinical synopsis
 |
| Figure 1 |
|---|
| Brownish dome-shaped papules with linear distribution |
A 23-year-old man treated with pegilated interferon-α for a chronic hepatitis C for the preceding 9 months was observed with small, brownish, dome-shaped papules distributed in a zosteriform pattern in the right submammary region (Fig. 1). The lesions arose 2 months previously and were clinically suggestive of lichen planus.
 |  |
| Figure 2 | Figure 3 |
|---|---|
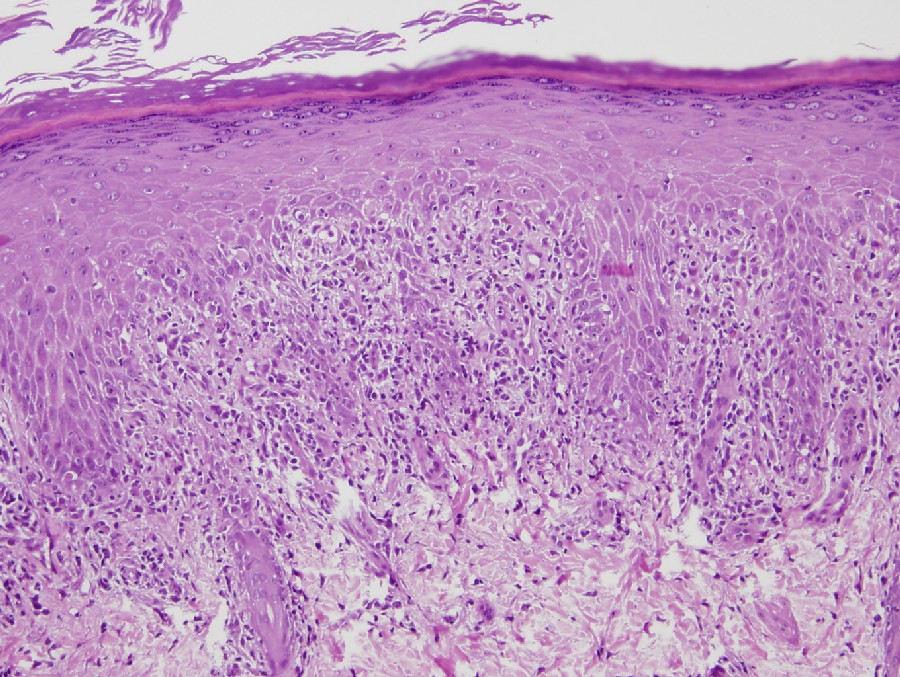
| Figure 2. Acanthosis, epidermal colloid bodies, and lichenoid mononuclear dermal infiltrate | |
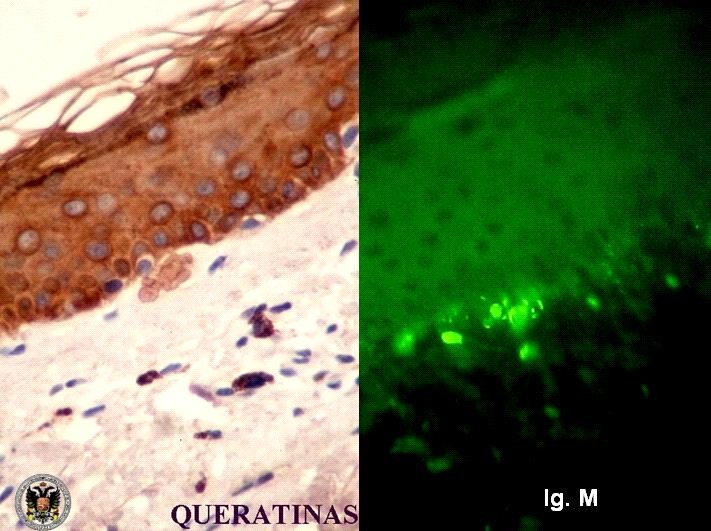
Figure 3. Immunocytochemical stain for cytokeratins and direct immunofluorescence revealing IgM deposition in the colloid bodies | |
Histopathology showed acanthosis, epidermal colloid bodies (cytokeratin-positive after immunocytochemical stain) and a lichenoid mononuclear dermal infiltrate, confirming the diagnosis (Figs. 2 and 3). Direct immunofluorescence revealed IgM deposition in the colloid bodies (Fig. 3).
The patient was successfully treated with topical 0.1 percent tacrolimus ointment once daily. However, during the following months he developed new flares of lesions distributed in a linear pattern, localized to the legs. A complete clinical response to topical tacrolimus was again obtained.
Discussion
The association of lichen planus and hepatitis C is well documented but the mechanism remains perplexing [5, 6]. Although several recent works claim that particles of hepatitis C virus are not found in lichen planus lesions [5], various authors defend this association [4, 6, 7, 8]. The role of interferon-α in the development of lichen planus is controversial. Several authors report that patients treated with interferon-α for hepatitis C do not develop lichen planus [8]. Conversely, reports of interferon-induced lichen planus are in the literature [8, 9, 10]. Based on a recent work performed involving patients with hepatitis C associated with lichen planus, an improvement of hepatitis was observed after interferon therapy, however the lichen planus showed no objective response to this drug [5].
This case appears to be the third description of the association of linear lichen planus and hepatitis C. We cannot conclude with certainty whether the lichen planus was triggered by hepatitis C or by interferon-α treatment.
Finally, we would like to emphasize the good response obtained with topical tacrolimus; as described for other forms of lichen planus, there was complete remission [11].
References
1. Herd RM, McLaren KM, Aldridge RD: Linear lichen planus and lichen striatus opposite ends of a spectrum. Clin Dermatol 1993;18:335-337. PubMed2. Mokni M, Rybojad M, Puppin D Jr, et al: Lichen planus and hepatitis C virus. J Am Acad Dermatol 1991;24:792. PubMed
3. Jury CS, Munro CS: Linear lichen planus related to hepatitis C infection? Br J Dermatol 2000;142:836-837. PubMed
4. Gunning MC, Turiansky G: Succesive linear, generalized, and oral lichen planus in a patient with chronic hepatitis C infection. J Am Acad Dermatol 2003;49:1190-1191. PubMed
5. Harden D, Skelton H, Smith K: Lichen planus associated with hepatitis C virus: No viral transcripts are found in the lichen planus, and effective theraphy for hepatitis C virus does not clear lichen planus. J Am Acad Dermatol 2003;49:847-852. PubMed
6. Giménez-García R, Pérez-Castrillón JL: Lichen planus and hepatitis C virus infection. J Eur Acad Dermatol Venereol 2003;17:291-295. PubMed
7. Jubert C, Pawlotsky JM, Pouget F, et al: Lichen planus and hepatitis C virus related chronic active hepatitis. Arch Dermatol 1994;130:73-76. PubMed
8. Guijarro B, López AF, Hernández Vallejo G: Presence of lichen planus during a course of interferon alpha-2a therapy for a viral chronic C hepatitis. Med Oral 2001;6:358-363. PubMed
9. Areias J, Velho GC, Cerqueira R, Barbedo C, Amaral B, Sanches M, et al: Lichen planus and chronic hepatitis C: exacerbation of the lichen under interferon alpha-2a therapy. Eur J Gastroenterol Hepatol 1996;8:825-828. PubMed
10. Sassigneux P, Michel P, Joly P, Colin R: Eruptive mucocutaneous lichen planus during treatment of chronic hepatitis C with interferon alpha. Gastroenterol Clin Biol 1993;17:764. PubMed
11. Ruzicka T, Assmann T, Lebwohl M: Potential future dermatological indications for tacrolimus ointment. Eur J Dermatol 2003;13:331-342. PubMed
© 2006 Dermatology Online Journal