Persistent edematous-plaque photosensitivity observed with sitagliptin phosphate (Januvia®)
Published Web Location
https://doi.org/10.5070/D30d70k7b2Main Content
Persistent edematous-plaque photosensitivity observed with sitagliptin phosphate (Januvia®)
Sherea M Stricklin BA1, William V Stoecker MS MD1, Ryan K Rader BS1, Antoinette F Hood MD2, Jerome Z Litt MD3, Thomas P Schuman PhD4
Dermatology Online Journal 18 (2): 9
1. Stoecker & Associates, Rolla, Missouri2. Eastern Virginia Medical School Department of Dermatology, Norfolk, Virginia
3. Case Western Reserve University School of Medicine, Cleveland, Ohio
4. Missouri University of Science & Technology, Rolla, Missouri
Abstract
Photosensitivity to sitagliptin, a dipeptidyl peptidase-4 (DPP-4) inhibitor, is reported. No previous reports of photosensitivity to any DPP-4 inhibitors are known. Physical examination of the patient revealed edematous plaques confined to sun-exposed areas of the skin. An unusual finding in this case was the spongy sensation upon palpation of the plaques. Histopathology revealed parakeratosis and abundant eosinophils, supporting the clinical impression of cutaneous drug sensitivity. The eruption finally cleared, approximately two years after onset.
Case presentation
 |
| Figure 1 |
|---|
| Figure 1. Eruption in photosensitive distribution displaying dermal edema and excoriations on extensor arms and hands following initiation of treatment with sitagliptin phosphate (Januvia). |
A 65-year-old male with diabetes on oral antihyperglycemic therapy presented with an excoriated cutaneous eruption confined to the extensor forearms and hands in a photodistribution, from the short sleeve line distally, with more extensive involvement on the right arm (Figure 1). The eruption first appeared approximately two weeks after beginning sitagliptin phosphate (Januvia®, Merck & Co., Inc., Whitehouse Station, NJ) in September and was accompanied by severe pruritus and deep excoriations, recurring intermittently throughout the winter. The patient initially denied sunlight exposure. On further questioning, he admitted to brief, intermittent sunlight exposure during the winter months. He did not consider sunlight exposure as a vehicular passenger to be significant.
 |  |
| Figure 2a | Figure 2b |
|---|---|
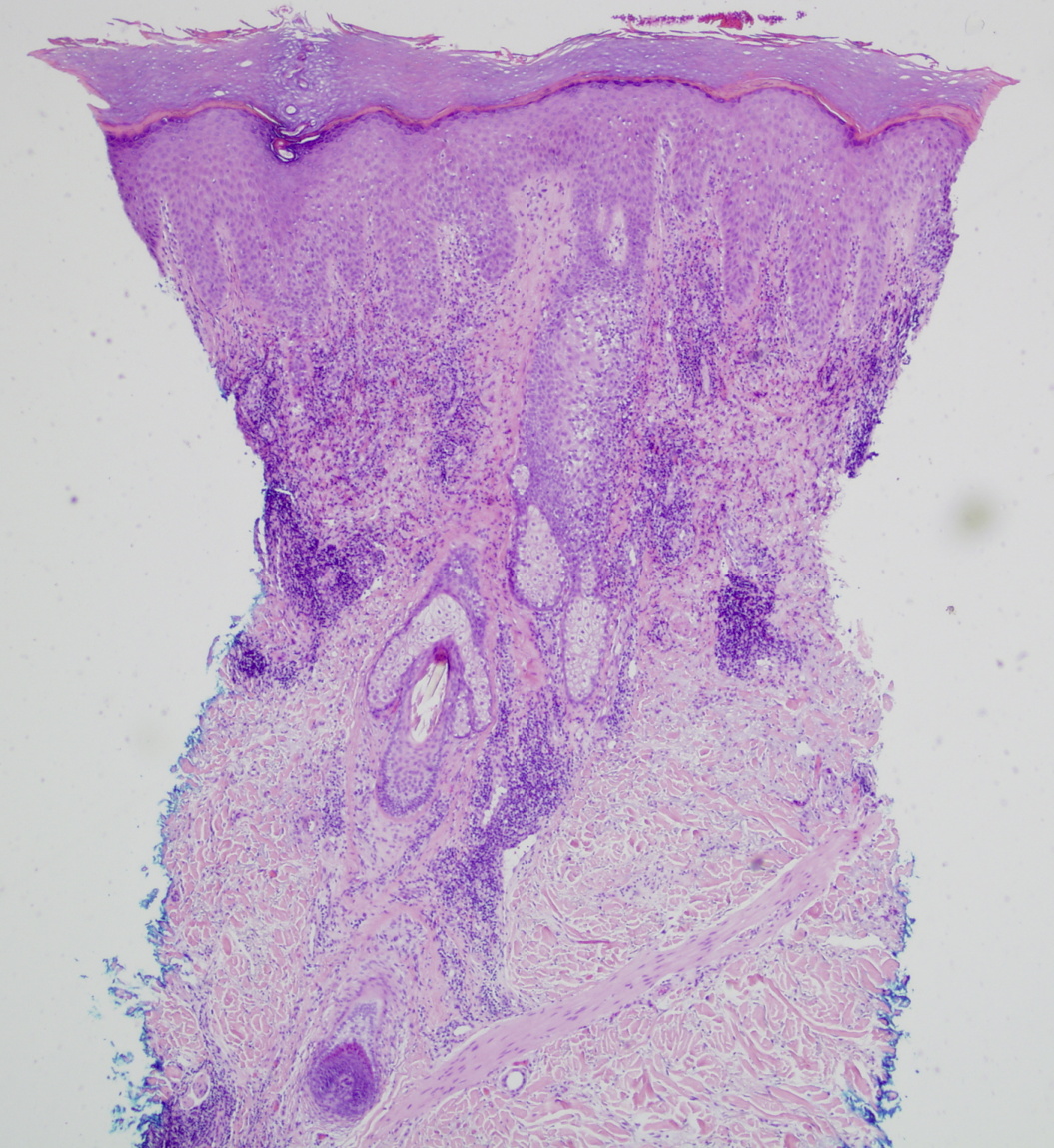
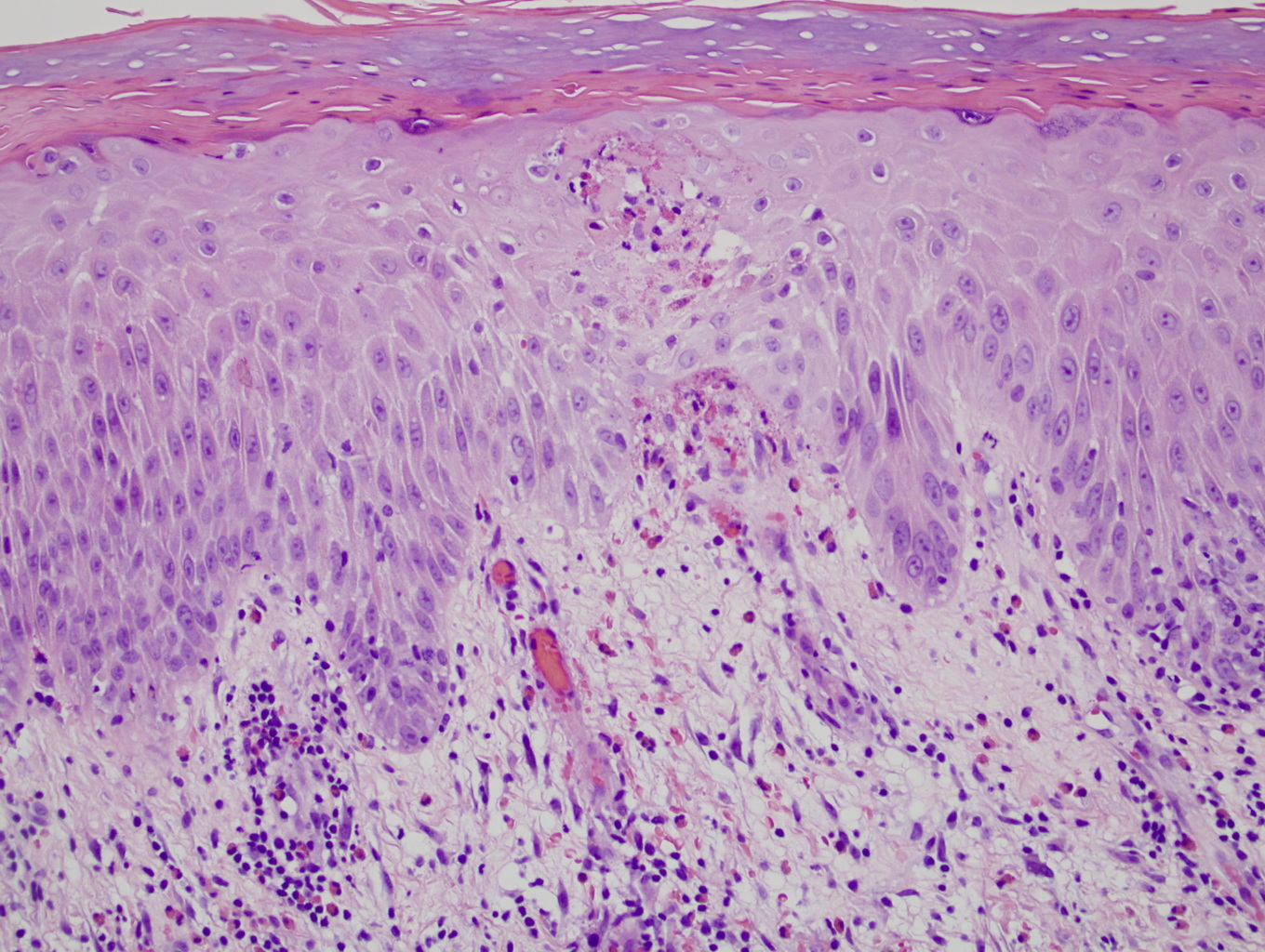
| Figure 2. Histopathology results (2a) 40x magnification and (2b) 200x magnification (H&E) | |
Examination showed excoriated plaques confined to the extensor forearms. A spongy, edematous sensation was appreciated upon palpation of the plaques. The histopathology obtained with punch biopsy with minimal lidocaine added at the sub-dermal level is shown in Figures 2a and 2b. The lower magnification (Figure 2a) displays scale-crust, orthokeratosis, and a superficial and mid-dermal mixed infiltrate. The higher magnification (Figure 2b) shows confluent parakeratosis below orthokeratosis and abundant eosinophils, confirming the clinical impression of cutaneous drug sensitivity. The patient was instructed to wear sunscreen and long sleeves anytime that he went outdoors or went riding in the car.
The sitagliptin therapy was discontinued by the primary care physician. Subsequent compliance to photoprotection measures was poor and the eruption continued on the arms for two years in the pattern noted above, confined to the sun-exposed forearms, with a greater involvement of the right arm. Photopatch testing at both 5 and 10 Joules was negative [1].
The patient was instructed to further improve his photoprotection with daily application of a broad-spectrum sunscreen and year-round use of long sleeves, emphasizing sun protection while riding in his car. The eruption finally cleared, approximately two years after onset. The clinical and histopathologic features of an eczematous eruption with spongiosis and dermal edema, confined to the sun-exposed surfaces of the arms and hands, suggested a localized form of photosensitive eczema.
To further evaluate the case, the absorption spectrum of sitagliptin phosphate was determined using a Cary 50 UV-Visible Spectrophotometer 3.00 (Agilent Technologies, Santa Clara, California, USA) with a solution of 2 x 10-4 molar sitagliptin phosphate. The absorption spectrum revealed three absorption peaks: 199.9 nm (Absorbance = 3.198), 265.0 nm (Absorbance = 0.491, ε (molar absorptivity) = 24,550 L/mol*cm), and 400.1 nm (Absorbance = 0.091, ε = 4,550 L/mol*cm). Absorbances at 199.9 and 265.0 nm agree with those previously reported for stigaliptin phosphate [2]. Both of these absorbance wavelengths are within the ultraviolet C spectrum below 290 nm, which is the shortest wavelength in sunlight reaching the earth’s surface [3]. The presence of the 400.1 nm absorbance peak indicates that sitagliptin absorbs at the UVA – visible light boundary.
Discussion
Sitagliptin phosphate, saxagliptin hydrochloride (Onglyza®, Bristol-Myers Squibb Company, Princeton, NJ 08543 USA), and vildagliptin (marketed in Europe as Galvus, Novartis, Basel, Switzerland), belong to the dipeptidyl peptidase-4 (DPP-4) inhibitor class for hypoglycemic drugs [4]. Although the medical literature cites multiple case reports of photosensitivity with other hypoglycemic drugs [5, 6], no reports have appeared of photosensitivity related to a DPP-4 inhibitor [7]. One website has reported 10 cases of sitagliptin photosensitivitity [8]. However, these cases lacked physician documentation or biopsy confirmation. The package inserts for all three marketed DPP-4 inhibitors do contain reports of cases of rash and/or urticarial. However, no reactions are linked with exposure to ultraviolet light.
Our patient had AN eczematous dermatitis persisting in the initial area of photodermatitis even after the drug was discontinued. This finally resolved after compliance with careful photoprotection measures. Unlike the majority of cases of chronic actinic dermatitis, he had negative photopatch results to the implicated photosensitizer [9, 10, 11]. He did not have a reduction in minimal erythema dose to UVA, manifested either clinically or by phototesting. He had no history of previous contact dermatitis and lacked the typical findings of generalized light sensitivity involving face, neck, and sun-exposed V-area of the chest, described classically by Hawk and Magnus, and usually found in recent series of chronic actinic dermatitis [9, 10, 11, 12].
The mechanism of persistent light sensitivity in an area of previous photosensitivity is not completely understood [10, 13, 14]. It has been theorized that induction of the UVA-dependent covalent binding of hapten, in this case sitagliptin, to endogenous protein occurs and photosensitivity is followed by chronic sensitivity to UVA in the absence of the hapten [10]. An in vitro model for chronic actinic dermatitis has been demonstrated with tetrachlorosalicylanilide, which is associated with chronic actinic dermatitis [15].
 |  |
| Figure 3a | Figure 3b |
|---|---|
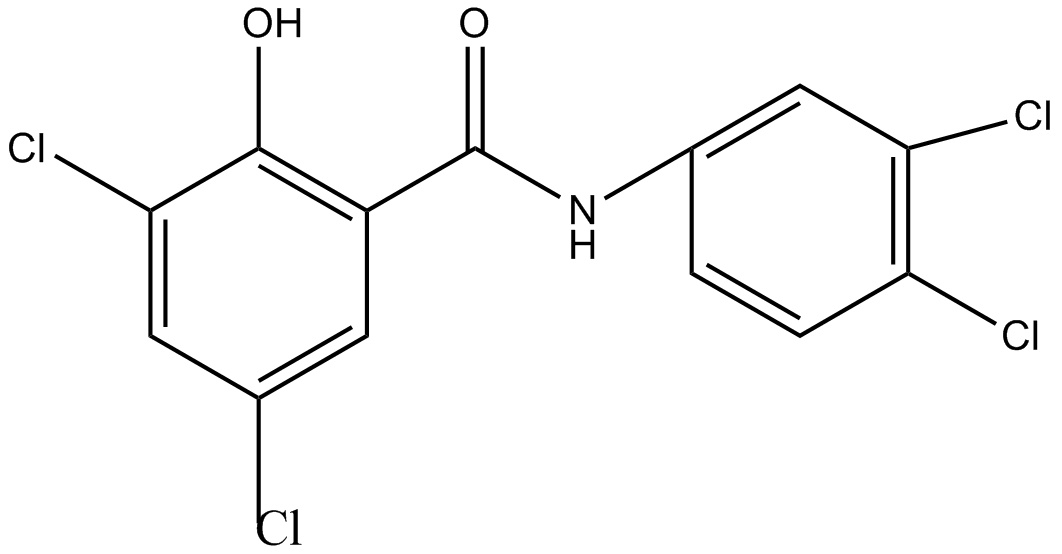
| Figure 3. Structures of known and postulated photosensitizing drugs (3a) Tetrachlorosalicylanilide, known photosensitizer (3b) Doxycycline, known photosensitizer (3c) Sitagliptin, proposed photosensitizer | |
 |
| Figure 3c |
|---|
The known photosensitizers, tetrachlorosalicylanilide and doxycycline, as well as the proposed photosensitizer, sitagliptin, all have a substituted phenyl ring and a carbonyl group (oxygen atom double bonded to a carbon atom), (Figures 3a, 3b, and 3c). Study of additional cases of photosensitivity from sitagliptin and other dipeptidyl peptidase-4 (DPP-4) inhibitors may help us understand the spectrum of photosensitivity from this DPP-4 inhibitor drug class.
In summary, our case is consistent with persistent photosensitivity related to sitagliptin phosphate. Because the eruption was confined to sun-exposed areas, and present during the winter months at a latitude of 37° N, it is clinically consistent with photosensitivity primarily related to ultraviolet A radiation. The greater involvement on the right arm is consistent with a significant ultraviolet A exposure while riding as a passenger in his car. The finding of spongiosis and significant dermal edema, appearing to comprise up to one-half of the dermal volume in areas, correlates with the unusual spongy and edematous sensation appreciated clinically. Plaques with substantial dermal edema in cases of chronic actinic dermatitis have been called “juicy plaques” [12]. This clinical finding should suggest chronic photosensitivity. When evaluating edematous plaques, clinicians performing a biopsy are cautioned to use small amounts of local anesthetic infiltrated at the sub-dermal level to avoid the addition of excess fluid at the level of the dermis. When communicating with patients who have drug-induced or other photosensitivity, a substantial educational effort to minimize exposure to ultraviolet radiation, in the car as well as outdoors, may be required.
References
1. British Photodermatology Group. Photopatch testing--methods and indications. Br J Dermatol. 1997 Mar;136(3):371-6. [PubMed]2. Pathade, P., Imran, Md., Bairagi, V., Ahire, Y., Development and Validation of Stability Indicating UV Spectrophotometric Method for the Estimation of Sitagliptin Phosphate in Bulk and Tablet Dosage Form, Journal of Pharmacy Research. 2011;4(3):871-873.
3. Farmer KC, Naylor MF. Sun exposure, sunscreens, and skin cancer prevention: a year-round concern. Ann Pharmacother. 1996 Jun;30(6):662-73. [PubMed]
4. Palalau AI, Tahrani AA, Piya MK, Barnett AH. DPP-4 inhibitors in clinical practice. Postgrad Med. 2009;121(6):70-100. [PubMed]
5. Kastalli S, El Aïdli S, Chaabane A, Amrani R, Daghfous R, Belkahia C. [Photosensitivity induced by metformin: a report of 3 cases]. Tunis Med. 2009;87(10):703-5. [PubMed]
6. Sun CC. Photosensitivity due to glyburide. Photodermatol. 1988;5(1):42-5. [PubMed]
7. Litt JZ. Drug Eruptions and Reactions Manual. 16th Edition. London, Informa. 2010
8. "Photosensitivity Reaction in Januvia, Reported by 8 People - EHealthMe.com." EHealthMe - Real World Drug Outcomes. http://www.ehealthme.com/ds/januvia/photosensitivity+reaction, accessed December 20, 2011.
9. Que SK, Brauer JA, Soter NA, Cohen DE. Chronic actinic dermatitis: an analysis at a single institution over 25 years. Dermatitis. 2011 Jun;22(3):147-54. [PubMed]
10. Somani VK. Chronic actinic dermatitis-a study of clinical features. Indian J Dermatol Venereol Leprol 2005;71:409. [PubMed]
11. Chew AL, Bashir SJ, Hawk JL, Palmer R, White IR, McFadden JP. Contact and photocontact sensitization in chronic actinic dermatitis: a changing picture. Contact Dermatitis. 2010 Jan;62(1):42-6. [PubMed]
12. Hawk JLM, Magnus IA. Chronic actinic dermatitis-an idiopathic photosensitivity syndrome including actinic reticuloid and photosensitive eczema. Br J Dermatol 1979;101(Suppl 17):24. [PubMed]
13. Booth AV, Mengden S, Soter NA, Cohen D. Chronic actinic dermatitis. Dermatol Online J 2008 May 15;14(5):25. [PubMed]
14. Hawk JLM. Chronic actinic dermatitis. Photodermatol Photoimmunol Photomed 2004;20:312. [PubMed]
15. Kochevar IE, Harber LC. Photoreactions of 3, 3’, 4’, 5-tetrachlorosalicylanilide with proteins. J Invest Dermatol 1977;68:151. [PubMed]
© 2012 Dermatology Online Journal