Generalised linear scleroderma in childhood
Published Web Location
https://doi.org/10.5070/D309p8v47mMain Content
generalized linear scleroderma in childhood
Vandana Mehta MD DNB, C Balachandran MD, Sunaina Hameed MD
Dermatology Online Journal 13 (3): 34
Department of Skin and STD , Kasturba Medical College, Manipal, Karnataka 576104, India.Linear morphea is a disease of unknown etiopathogenesis occurring most commonly in children. It is characterized by linear, indurated plaques along the length of a limb or occasionally by band-like lesions leading to pseudoainhum. The plaques are usually single and unilateral in distribution. However, bilateral lesions have been reported [1]. The plaques of linear morphea are said to follow the lines of Blaschko, although it has been a matter of dispute [2]. We report an unusual case of linear morphea involving all the limbs with an overlapping of various subtypes of morphea in the same patient.
Clinical synopsis
A 6 year-old girl presented with linear hyperpigmented, indurated plaques on the upper and lower extremities of 9 months duration The onset followed a febrile illness that was diagnosed as typhoid. The lesions extended to involve the trunk and followed a wavy pattern. There was no history of trauma, excessive physical exertion, or Raynaud phenomenon. She had no systemic complaints. Upon physical examination, there was wasting of the left upper and lower limbs with a painful toe stepping gait due to contracture at the left ankle. Routine hematological and biochemical investigations were normal. Anti DsDNA and anti histones were positive. Biopsy for histopathology showed features consistent with morphea.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Wavy hyperpigmented indurated plaques on the trunk Figure 2. Indurated hyperpigmented plaques on the lower extremities | |
 |  |
| Figure 3 | Figure 4 |
|---|---|
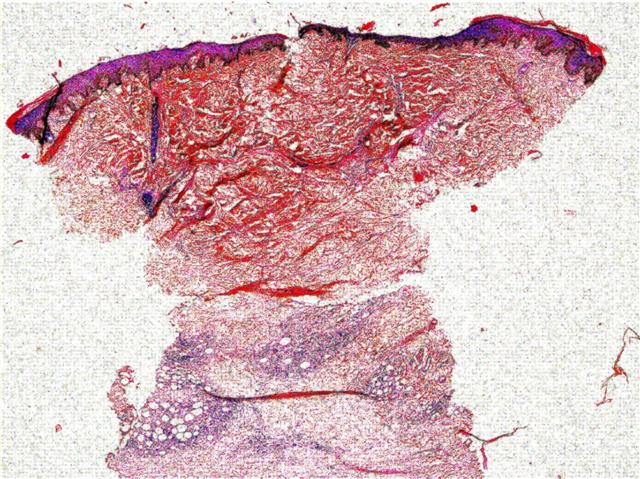
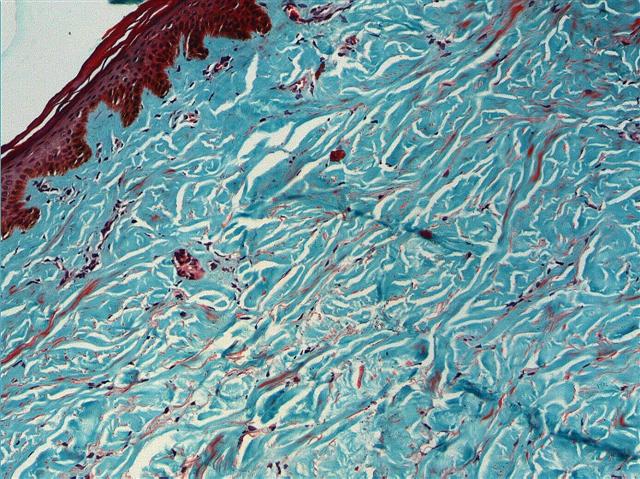
| Figure 3. Photomicrograph demonstrating homogenization of dermal collagen Figure 4. Masson trichrome stain showing the homogenized collagen bundles | |
Comment
The exact cause of linear morphea is unknown however trauma, excessive physical exertion, immobilization, radiation, infection by Borrelia burgdorferi, febrile illness, and vaccinations have been proposed as trigger factors. Generalized morphea occurs when morphea plaques become confluent and affect a significant proportion of three or more major anatomical regions. Disabling pansclerotic morphea is a rare atrophying and sclerosing disorder seen in children younger than 14 years that affects the subcutaneous tissue, muscles, tendons, and even bones. It may develop from linear morphea and has a relentless, mutilating course leading to complications that include contractures, deformities, ulcers, and even squamous cell carcinoma [3, 4].
A childhood onset occurs in 2-3 percent of all cases of scleroderma. The clinical features are essentially similar to adults however a prior history of trauma is usually present in 25 percent of children. Children are also less likely to show serological abnormalities as compared to adults; ANA is positive in one third of those with localized disease [5]. Linear morphea and generalized morphea both show ANA positivity in 30-50 percent of the cases.
Our patient exhibits a rare presentation that does not fit well into the morphea classification proposed by Peterson et al. [6]. There was rapid progression to extensive and symmetrical involvement of all the limbs in a relatively short span. The truncal involvement indicates a progression to generalized morphea that was perhaps precipitated by the febrile illness. The contracture at the ankle and wasting of muscles may indicate the possibility of future extension to pansclerotic morphea. The extensiveness of her disease is complimented by positive anti-DsDNA and anti histone serologies that are indicative of the disease activity [7, 8]. Our patient received oral corticosteroids in a dose of 10mg/day for a period of 4 months, intralesional steroids on two occasions into the indurated plaques, and physiotherapy. Progression of the induration has ceased and the plaques have softened.
References
1. Leigh EE, Elizabeth IM, Wesley G, Richard R. Linear Scleroderma in Children. Int J Dermatol 1996; 35:330-62. Hauser C, Skaria A , Harms M , Saurat JH. Morphea following Blaschko's lines. Br J Dermatol 1996;134:593-4.
3. Jose L , Suzanne MC, Winkelmann RK. Diabling Pansclerotic Morphea of children. Arch Dermatol 1980; 116: 169-73.
4. Padmavathy L , Rao L . Unilateral linear pansclerotic morphea affecting face and limbs. Indian J Dermatol Venereol Leprol 2005;71:192-4
5. Rosenberg AM, Uziel Y, Krafchik BR. Antinuclear antibodies in children with localized scleroderma. J Rheumatol 1995;22: 2337-43.
6. Peterson LS, Nelson AM, Su WP. Classification of morphea ( localized scleroderma ). Mayo Clin Proc 1995;70: 1068-76.
7. ElAzhary RA, Aponte CC, Nelson AM. Do antihistone autoantibodies reflect disease activity in linear morphea? Arch Dermatol 2004;140: 759-60.
8. Falanga V , Medsger TA , Reichlin M. Antinuclear and anti- single stranded DNA antibodies in morphea and generalized morphea . Arch Dermatol 1987;123: 274-9.
© 2007 Dermatology Online Journal