
Yellow plaques and papules on the skin are hallmarks of xanthomas. These are not always associated with abnormalities in lipid profiles or their associated proteins. In cases of diffuse normolipemic plane xanthomas these cutaneous findings are often associated with myelodyscrasias including monoclonal gammopathy of unknown significance and multiple myeloma. Such clinical presentations may indicate that an evaluation for myelodyscrasias is warranted.
|
|
| Figure 1 | Figure 2 |
|---|
An 80-year-old white male presented for evaluation of a six-year history of slowly increasing yellow skin lesions. He had no significant past medical history nor a family history of hypercholesterolemia or early cardiac deaths. He denied systemic complaints such as shortness of breath or chest pain.
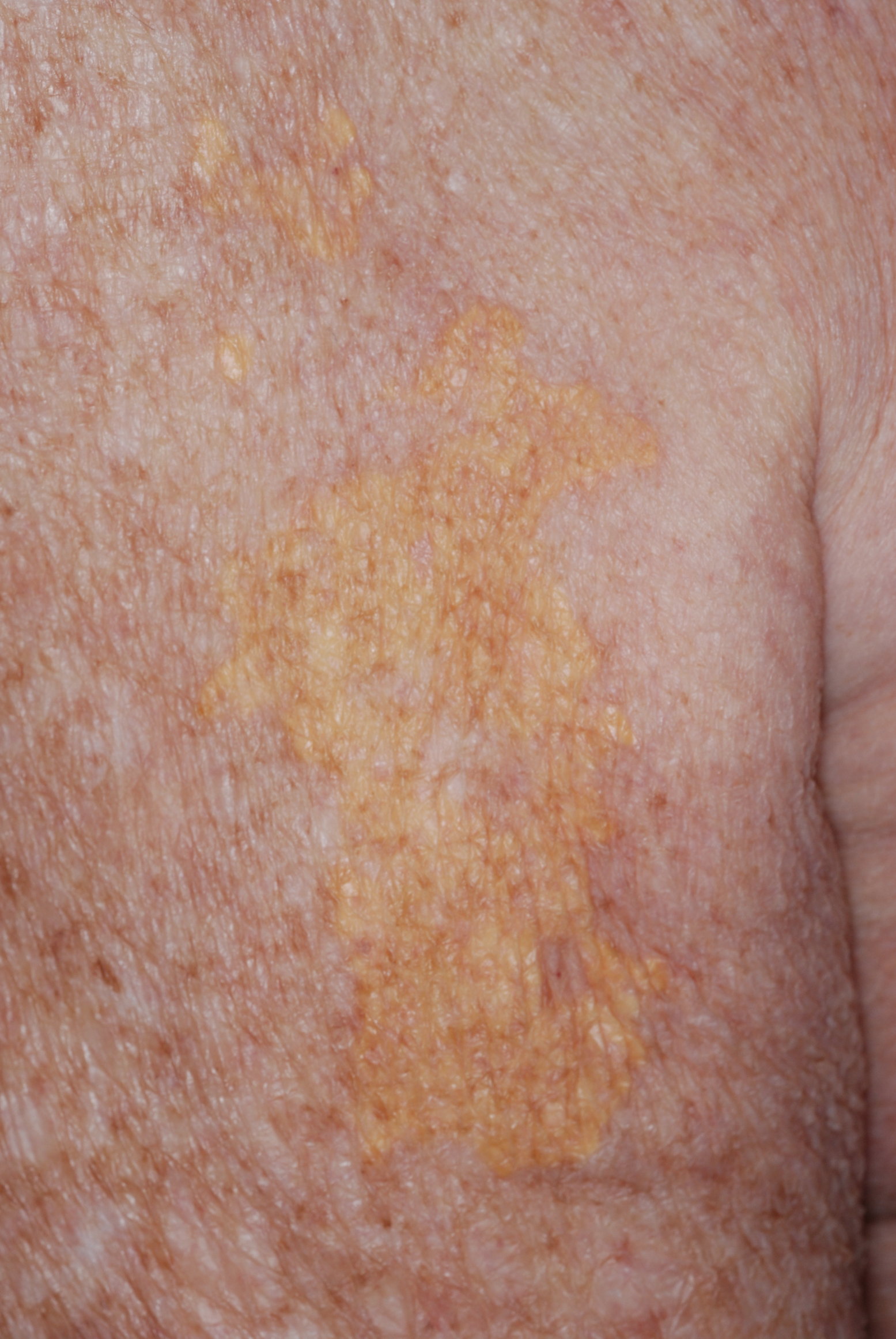
On skin examination, a yellow papule near the lateral epicanthus and a yellow macule near the temple were present (Figure 1). Multiple, well-demarcated yellow skin plaques in sheets were noted on the arms and back (Figure 2). There was no involvement of his palms, tendon areas, or other parts of his skin.
 |
 |
| Figure 3 | Figure 4 |
|---|
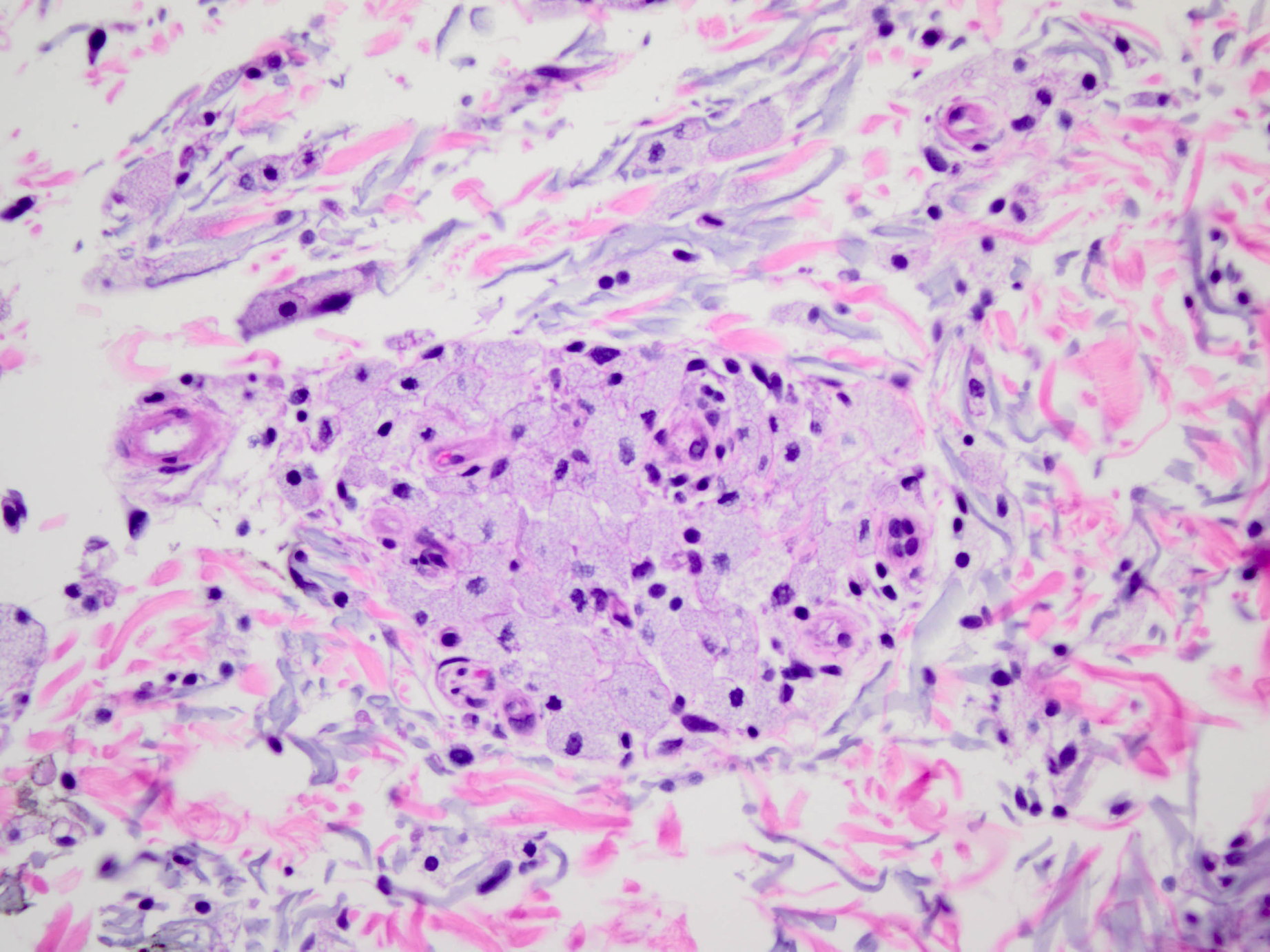
Laboratory studies demonstrated normal electrolytes, calcium, creatinine, liver function tests, and lipid studies. Serum hemoglobin was low at 11.8. Platelet count and white blood cell count were normal. An intralesional skin biopsy was obtained for a Hematoxylin-Eosin (H&E) stain (Figures 3 and 4).
The biopsy demonstrated proliferation of foamy macrophages within the dermis without necrosis or palisading (Figures 3 and 4). The overlying epidermis was unremarkable. Urine tests revealed increased protein, predominately Bence-Jones proteins. Serum protein immune-electrophoresis revealed IgG kappa paraproteinemia. No lytic lesions were seen on radiography. A bone marrow biopsy was performed showing 10 percent plasma cells, which ultimately yielded a diagnosis of smoldering or incipient multiple myeloma (MM).
Diffuse normolipemic plane xanthomas (DNPX) are an uncommon occurrence mainly affecting adults and are associated with blood dyscrasias especially monoclonal gammopathy [1, 2]. Since the original description in 1965 a strong association of DNPX with systemic disorders, especially MM and monoclonal gammopathy, has been established. Other disorders have also been reported in association with DNPX, including leukemia and Castleman disease.
The first xanthomatous plaques typically appear on the face or palpebral area and exhibit the potential for slow cutaneous progression. Hallmarks of DNPX are sheet-like xanthomas, also known as plane xanthomas, of the head, neck, trunk, and extremities. They usually present symmetrically on the body surface. Palpebral xanthelasma may also be present, but lipid levels and cholesterol are characteristically normal. On histopathology, the characteristic findings are foam cells, which are lipid-laden macrophages. There is typically no family history of significant lipid or cholesterol abnormalities. Additional cholesterol studies can be performed, such as lipoprotein A or cholesterol receptor analyses; however, these are normal.
The pathogenesis of DNPX has been attributed to the formation of complexes of monoclonal IgG and low-density lipoprotein with deposition in the skin and subsequent phagocytosis by histiocytes [3, 4]. Complement level abnormalities have also been attributed to the development of DNPX [5, 6]. Purpura and petechiae may present if immune complex aggregates lead to vasculitis. For limited cutaneous involvement, cosmetic excision, dermabrasion, or ablative laser therapy are options [2, 3]. For diffuse disease, treatment options are limited.
This disorder is important to consider in rare cases of cutaneous xanthomatous plaques in which lipid profiles are unremarkable and there is no family history of lipid profile abnormalities or cardiovascular events occurring at young ages. Such a patient may require further evaluation for hematologic malignancies.
ACKNOWLEDGEMENTS: We would like to thank Robert Jordon MD for his mentorship and expert input on the manuscript and Scott Bangert MD for his dermatopathology expert assistance.
© 2011 Dermatology Online Journal