Unknown: Two adjacent nodules on the leg
Heleen D de Koning MD, H Jorn Bovenschen MD PhD
Dermatology Online Journal 16 (6): 13
Department of Dermatology, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands. j.bovenschen@derma.umcn.nl
Abstract
Poroma is a rare benign neoplasm (derived from the intraepidermal part of the eccrine or apocrine duct), which may clinically
mimic malignant tumors such as (amelanotic) malignant melanoma and porocarcinoma. Histopathological examination is the key
to the correct diagnosis, which is illustrated in the present case, in which a pigmented basal cell carcinoma and a poroma
are in close proximity to each other. Despite a clinical differential diagnosis of melanoma, histopathology showed the typical
characteristics of a poroma, a rare but much more favorable tumor. Histopathological features of poroma are discussed.
Answer: Poroma (Arrow) and pigmented nodular basal cell carcinoma (Arrowhead)
 |
 |
| Figure 1 |
Figure 2a |
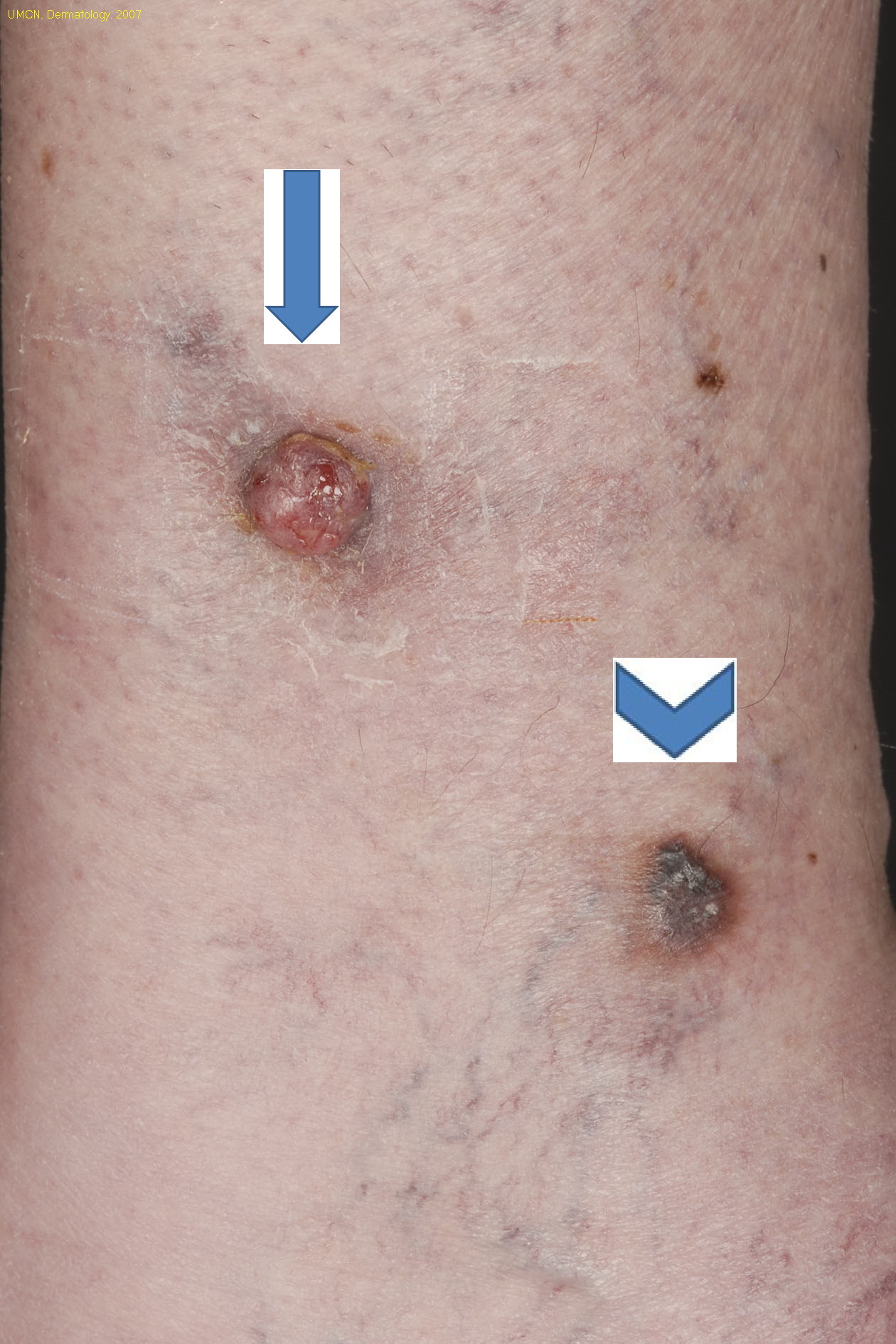
Figure 1. (Arrow) Painful erythematous teleangiectatic nodule (diameter 12 mm), with a nearby (Arrowhead) sharply demarcated
hyperpigmented nodule (diameter 10 mm) on the left lower leg
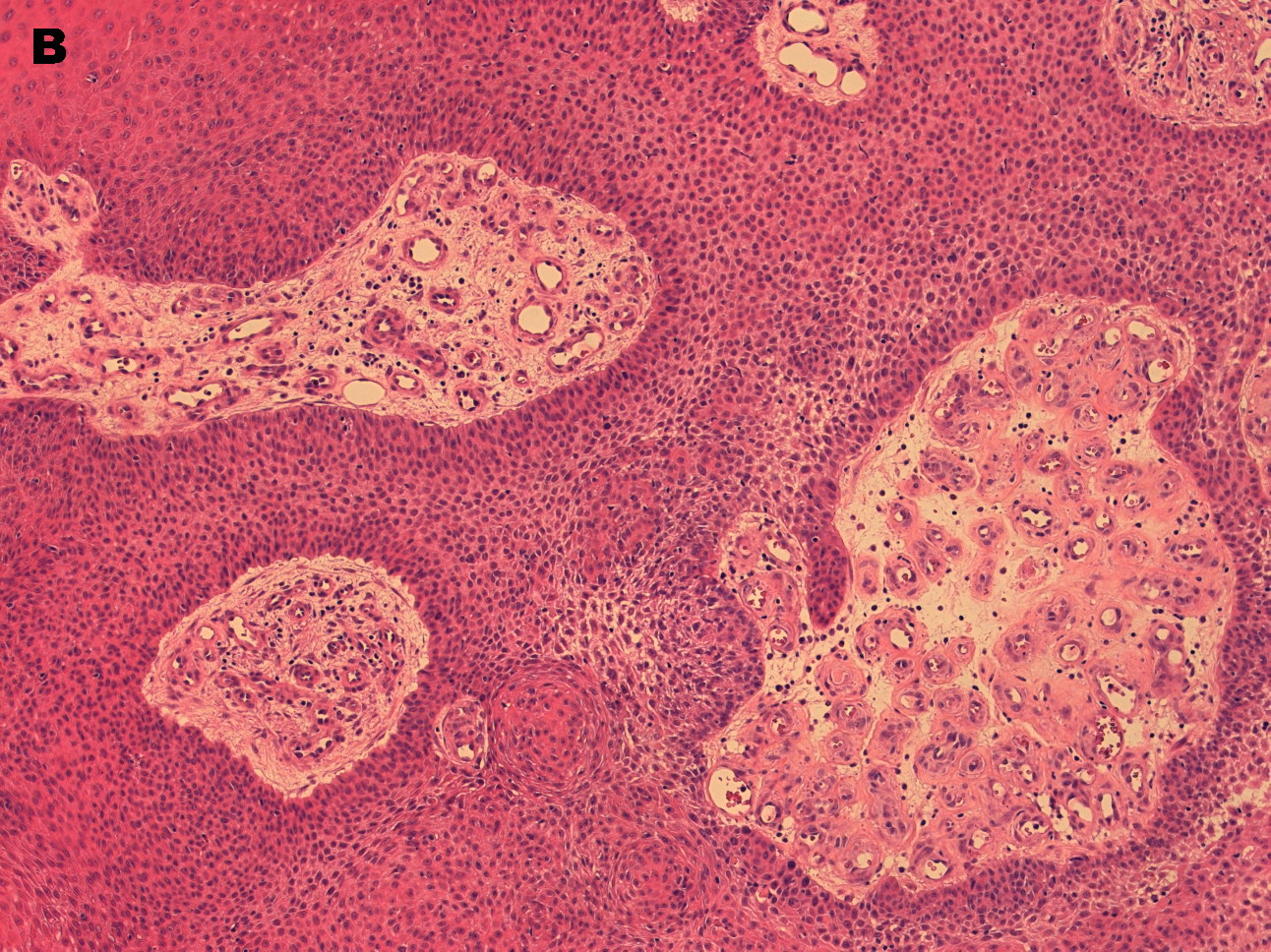
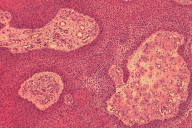
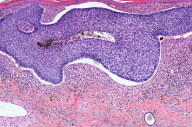
Figure 2. Histology of the upper lesion (Arrow) showed a polypoid exophytic tumor with acanthosis of the epidermis and lumina
with surrounding cylindrical epithelial cells. Comparable nests of epithelial ‘poroid’ cells with tubular differentiation
and lumina were observed in the dermis, presenting as inter-anastomosing cords. There was an abundance of small vessels in
and around the tumor, a fibrous eosinophil stroma reaction and a small infiltrate containing lymphocytes and plasma cells.
The tumor reached to the level of the sweat glands and there were especially no signs of infiltration. (H&E, 2a: x50 and 2b:
x100). |
 |
 |
| Figure 2b |
Figure 3 |
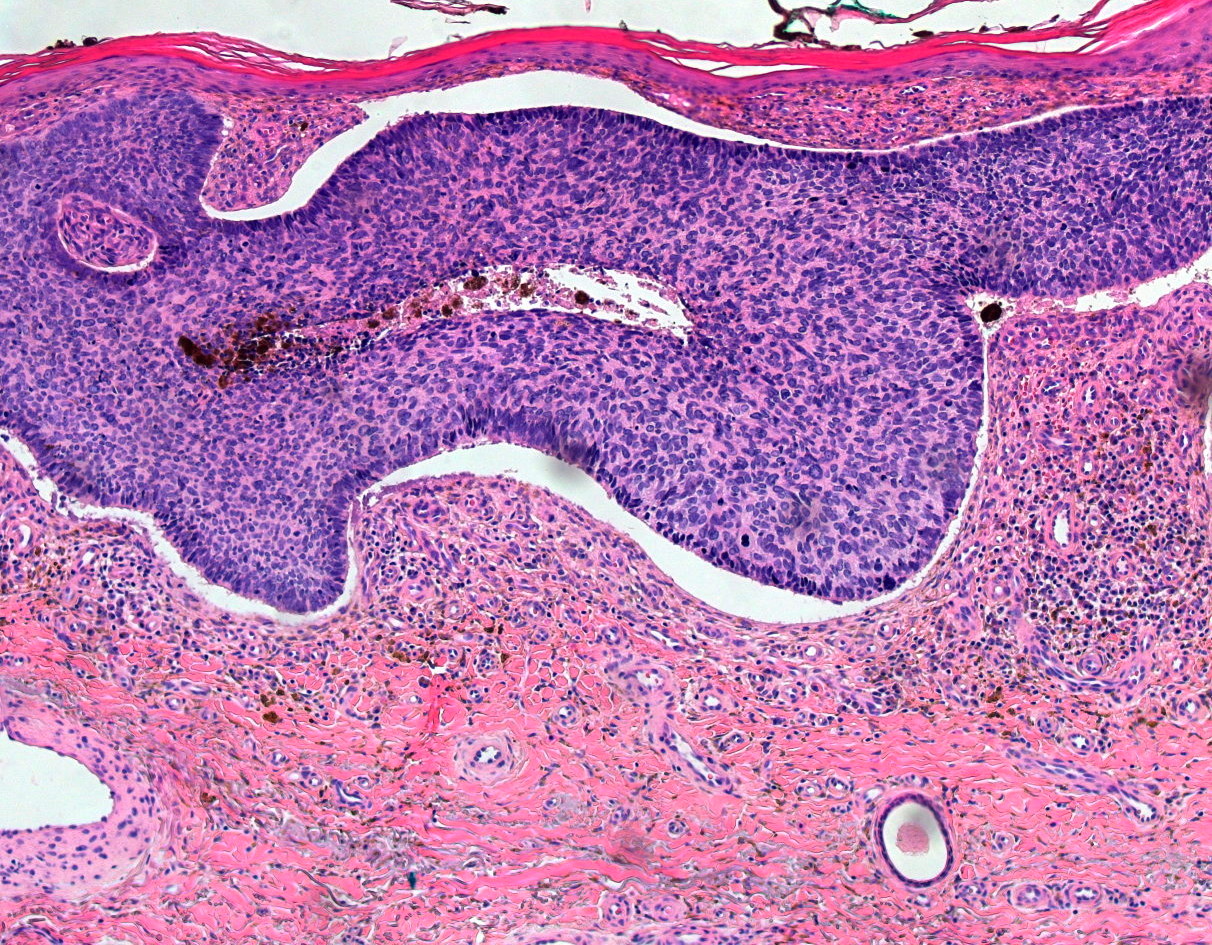
| Figure 3. The lower lesion (Arrowhead) was histopathologically clearly consistent with a pigmented basal cell carcinoma, with
atypical basaloid cells, retraction artefact, peripheral palisading basal cells, and an abundance of pigment. (H&E, x100) |
A 62-year-old otherwise healthy Caucasian woman presented with a painful, exsudative, easily bleeding erythematous telangiectatic
nodule on the medial side of her left lower leg, which had steadily grown over the past three years (Arrow) (Figure 1). Just
below she had a tender indurated nodule with hyperpigmentation (Arrowhead). Both lesions were excised and histopathological
findings of the lesions are depicted in Figures 2 and 3, respectively.
Histopathological findings
The clinical differential diagnosis in this case included (I) (amelanotic) melanoma, pyogenic granuloma and squamous cell
carcinoma, and for (II): melanoma, satellite metastasis, dysplastic nevus, or pigmented basal cell carcinoma. The diagnosis
is generally made by means of histopathology.
Histology of the excision of the upper lesion (Arrow) showed a polypoid exophytic tumor with acanthosis of the epidermis with
a non-atypical basal cell proliferation (Figure 2A). In between, lumina with surrounding cylindrical epithelial cells were
detected. Comparable nests of epithelial “poroid” cells with tubular differentiation and lumina were observed in the dermis,
presenting as inter-anastomosing cords. There was an abundance of small vessels in and around the tumor. Some fibrous, eosinophil
stroma reaction with some amyloid deposition was seen. The small infiltrate contained lymphocytes and plasma cells. The tumor
reached to the level of the sweat glands and there were no signs of infiltration (Figure 2B). There was no nuclear atypia
or dysplasia and only few mitotic figures were present. Immunoperoxidase staining of carcinoembryonic antigen (CEA) was positive
for several lumina in the tumor, whereas the epithelial membrane antigen (EMA) was less obviously positive. PAS-positive material
was observed. It was concluded that the histopathology was typically in line with a poroma. On histopathological examination,
the lower (Arrowhead) appeared to be a pigmented nodular basal cell carcinoma (Figure 3).
Discussion
In this case, both tumors presented in close proximity to one another, which raised a strong suspicion of malignant melanoma.
Because basal cell carcinoma is a well-established tumor in the differential diagnosis of melanoma, only the poroma will be
further discussed here. Poroma is a rare benign neoplasm derived from the intraepidermal part of the eccrine or apocrine duct.
Exact prevalence numbers are unknown. Eccrine poromas mainly arise on plantar, palmar, and plantar skin, but in a large series
the head was affected in 40 percent of the cases [1, 2]. In fact, any skin area containing sweat glands can be affected. Recent studies have shown that poromas can be of either
eccrine or apocrine lineage, the latter being even more common. A keratin expression study found that eccrine poromas are
pure periductal sweat gland tumors derived from the basal keratinocytes of the eccrine duct ridge and the lowermost acrosyringium
[3]. The etiology is largely unknown, but associations with scarring, radiation and trauma have been reported [4, 5, 6]. It usually appears in middle-aged or elderly people as a solitary lesion, but the tumors may occur in clusters (poromatosis)
[1]. Lesions are usually asymptomatic although pain has been reported. Poromas have a heterogenic appearance, but most of them
typically present as a sharply demarcated, soft erythematous 2 to 12 mm papule or nodule that may be sessile or pedunculated
[7, 8]. In general, malignant (amelanotic) melanoma, porocarcinoma, and non-melanoma skin cancer, such as squamous cell carcinoma
and Merkel cell tumor must be excluded [9].
Epiluminescence findings show a considerable heterogeneity ranging from polymorphous vascular patterns with pin-point, hairpin
vessels and/or arborizing vessels, to blue-gray ovoid nests and blue-gray dots [8, 10]. Because these findings are commonly observed in skin cancers, they do not discriminate between poroma and malignant (amelanotic)
melanoma, non-melanoma skin cancer or porocarcinoma. Therefore, epiluminescent examination of poroma has little diagnostic
significance and histological examination is indispensable for making the correct diagnosis [8, 10, 11].
Surgical excision of the entire lesion is warranted if a malignancy is suspected; small biopsy specimens may falsely appear
benign in the case of a porocarcinoma, the malignant counterpart of poroma [12]. It is important to distinguish between these two entities because malignant porocarcinoma can metastasize and cause death.
Clinical signs of porocarcinoma include bleeding, pain, and pruritus, whereas poromas are mostly asymptomatic. Histologically,
cytologic atypia and infiltration of poroid cells distinguish malignant porocarcinoma from eccrine poroma [12]. Differences may be very subtle. Malignant transformation of poroma into porocarcinoma has been described, but is controversial.
However, in a series of 69 cases of porocarcinoma, 18 percent appeared to have arisen in continuity with a preexisting poroma
[12].
In conclusion, poroma is a rare benign tumor that may clinically mimic malignant tumors such as (amelanotic) malignant melanoma
and porocarcinoma. In the present case, the uncommon co-occurrence of poroma and pigmented basal cell carcinoma was a major
pitfall. Because the diagnosis is based on specific histopathological criteria surgical excision of the entire lesion is warranted
if a malignancy is suspected.
References
1. Ackerman AB, Abenoza P. Neoplasms with eccrine differentiation. Philadelphia: Lea & Febiger. 1990:113-85.
2. Moore TO, Orman HL, Orman SK, Helm KF. Poromas of the head and neck. J Am Acad Dermatol. 2001 Jan; 44(1):48-52. [PubMed]
3. Langbein L, Cribier B, Schirmacher P, et al. New concepts on the histogenesis of eccrine neoplasia from keratin expression
in the normal eccrine gland, syringoma and poroma. Br J Dermatol. 2008 Sep; 159(3):633-45. [PubMed]
4. Nemoto I, Akiyama N, Aoyagi S, et al. Eccrine porocarcinoma and eccrine poroma arising in a scar. Br J Dermatol. 2004 Jun;
150(6):1232-1233. [PubMed]
5. Penneys NS, Ackerman AB, Indgin SN, Mandy SH. Eccrine poroma: two unusual variants. Br J Dermatol. 1970; 82(6):613-615.
[PubMed]
6. Johnson RC, Rosenmeier GJ, Keeling JH 3rd. A painful step. Eccrine poroma. Arch Dermatol. 1992 Nov; 128(11):1530-1533.
[PubMed]
7. Jagdeo J, Robinson-Bostom L, Long T. Unusual clinical presentation of benign eccrine poroma. J Am Acad Dermatol. 2005 Apr;
54(4):733-734. [PubMed]
8. Altamura D, Piccolo D, Lozzi GP, Peris K. Eccrine poroma in an unusual site: A clinical and dermoscopic simulator of amelanotic
melanoma. J Am Acad Dermatol 2005 Sep; 53(3):538-540. [PubMed]
9. Roaf V, Chin N, Lynfield Y. Pigmented sweat gland tumor mimicking melanoma. Cutis 1997 Jan; 59(1):43-46. [PubMed]
10. Blum A, Metzler G, Bauer J. Polymorphous vascular patterns in dermoscopy as a sign of malignant skin tumors. A case of
an amelanotic melanoma and a porocarcinoma. Dermatology 2005; 210(1): 58-59. [PubMed]
11. Nicolino R, Zalaudek I, Ferrara G, et al. Dermoscopy of eccrine poroma. Dermatology. 2007; 215(2):160-163. [PubMed]
12. Robson A, Greene J, Ansari N, et al. Eccrine porocarcinoma (malignant eccrine poroma): a clinicopathologic study of 69
cases. Am J Surg Pathol. 2001 Jun; 25(6):710-720. [PubMed]
© 2010 Dermatology Online Journal